Key Takeaways
- Assessment Scoring Guide: Utilize the CIWA-Ar scale to dictate care levels: 0-8 (mild, outpatient possible), 9-15 (moderate, sub-acute residential), 16+ (severe, intensive medical monitoring required).
- Top 3 Success Factors: 1. 24/7 medical monitoring during the first 72 hours (reduces severe complication risk by up to 15%). 2. Seamless transition to Partial Hospitalization Programs (PHP) or Intensive Outpatient Programs (IOP), which increases 1-year success rates from 8% to 40%. 3. Utilizing data-driven software like ERPHealth to track statistically significant outcomes.
- Immediate Next Action: Evaluate your current patient’s risk window and match them to the appropriate level of care, whether that’s sub-acute detox or a home-like residential program.
Why Medical Supervision in Alcohol Detox Prevents Fatal Outcomes
The Neurobiology Behind Withdrawal Danger
- History of seizures or delirium tremens (DTs)
- Marked anxiety, tremors, or hallucinations within hours of last drink
- Rapid pulse, elevated blood pressure, or profuse sweating
- Co-occurring mental health conditions (depression, anxiety, PTSD)
Understanding why alcohol detox can be so dangerous starts with the brain. Chronic alcohol use disrupts the natural balance of neurotransmitters—chemical messengers that help your nerve cells communicate. When alcohol is suddenly removed, the brain struggles to regain equilibrium. This sudden shift can trigger what’s known as rebound excitation, where the nervous system becomes overactive.
That’s why withdrawal can lead to tremors, severe agitation, hallucinations, and—most critically—seizures or DTs, which can be fatal without rapid intervention. At Pacific Crest Trail Detox (PCTD), we emphasize a compassionate, home-like residential environment rather than a sterile hospital setting, ensuring individuals feel safe while receiving this critical medical oversight.
Deep Dive: Neurotransmitter Imbalance
Alcohol acts as a depressant by enhancing GABA (an inhibitory neurotransmitter) and suppressing NMDA (an excitatory neurotransmitter). During detox, the sudden absence of alcohol leaves the brain flooded with excitatory signals, causing the dangerous physical symptoms of withdrawal.
The risk isn’t just theoretical. Up to 15% of patients withdrawing from alcohol develop severe complications, including seizures and DTs, especially if medical supervision is lacking3. The danger is even higher for those with a long history of heavy alcohol use, prior withdrawal episodes, or underlying medical conditions.
Medical supervision allows for real-time monitoring of these neurobiological changes. By quickly recognizing warning signs, clinicians can intervene with evidence-based treatments and prevent neurological crises. This approach works best when the risk factors above are present, or when a patient has experienced complicated withdrawals in the past.
Yes, the science behind alcohol withdrawal is complex—and it’s completely normal to feel a bit overwhelmed. Remember: every day you prioritize safety, you’re protecting lives. Next, you’ll see how the timeline of withdrawal complications shapes clinical decision-making.
Timeline of Complication Risk Windows
| Time Since Last Drink | Primary Risk Window & Symptoms to Monitor |
|---|---|
| First 6–12 hours | Watch for mild agitation, tremors, headache, nausea. |
| 12–48 hours | Highest risk for seizures, worsening vital signs, hallucinations. |
| 48–72 hours | Monitor closely for delirium tremens (DTs)—confusion, fever, cardiovascular instability. |
| After 72 hours | Risk tapers but can persist for severe cases, especially with co-occurring illness. |
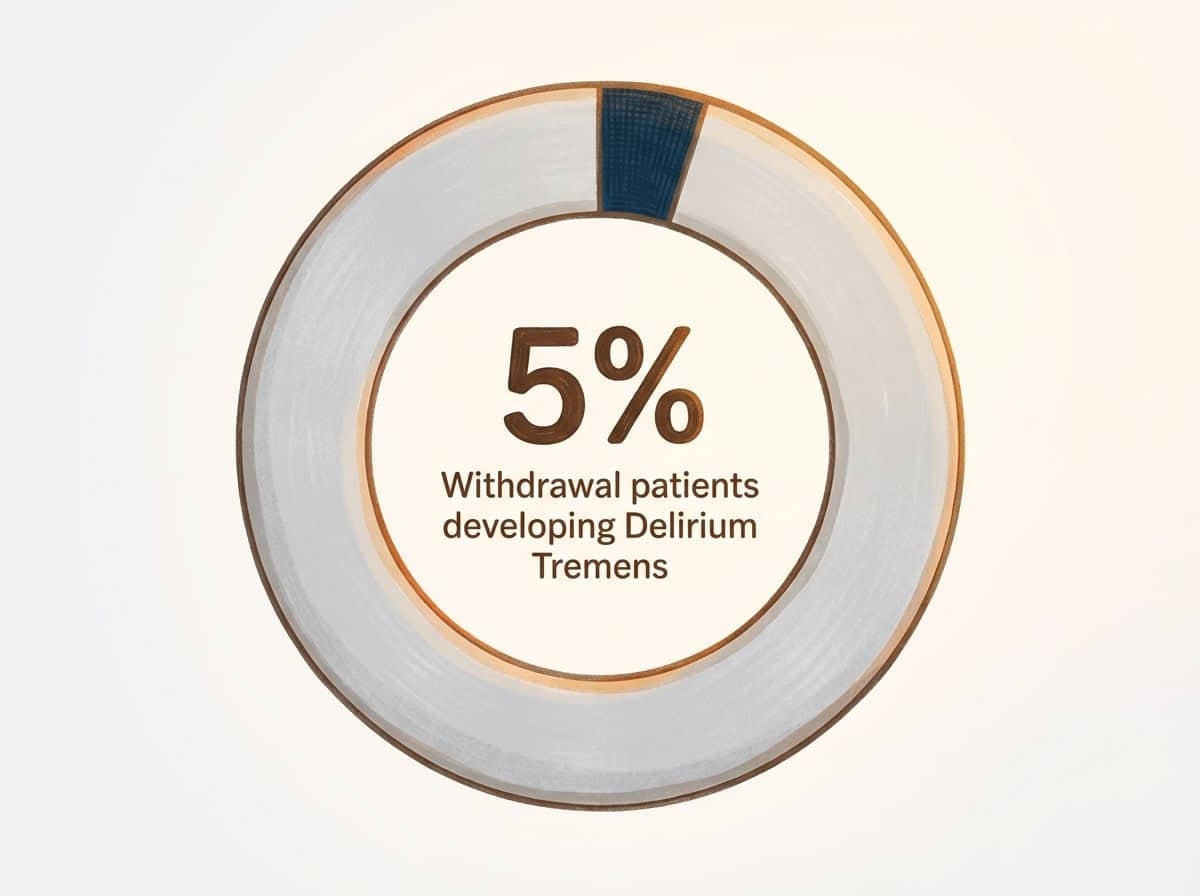
Understanding the timeline of complication risk windows helps you anticipate and respond to each phase with clarity. Symptoms of withdrawal can start as early as 6 hours after the last drink and may peak with life-threatening events—like seizures or DTs—between 24 and 72 hours3. In fact, delirium tremens develops in about 5% of hospitalized withdrawal cases, with mortality reaching up to 5% if not managed promptly3.
Consider this method if you’re managing individuals with a history of heavy use, repeated detox attempts, or other medical vulnerabilities. Early, continuous monitoring is especially critical during the first 48 hours, when most severe complications arise. If you’re supporting a patient past the 72-hour mark with no major symptoms, that’s a significant milestone—every hour of stability is progress worth celebrating!
Yes, the watchful waiting can feel tense, but your vigilance saves lives. Being present and prepared during each risk window ensures that complications don’t escalate unnoticed. Now that you have a clear sense of when the greatest dangers emerge, the next step is comparing evidence-based medication protocols to match the right intervention with each stage.
Evidence-Based Medication Protocols for Alcohol Detox
Benzodiazepine Dosing Strategies Compared
- Symptom-triggered: Use if patient is alert, able to communicate, and suitable for frequent assessment (CIWA-Ar monitoring).
- Fixed-schedule: Consider if patient has history of complicated withdrawal, cognitive impairment, or limited access to ongoing assessment.
- Front-loading: Opt for severe withdrawal with high seizure risk, when rapid stabilization is needed.
Benzodiazepines are the cornerstone of withdrawal management, but how you dose them makes a world of difference in patient outcomes. Symptom-triggered dosing—where medication is given based on real-time withdrawal scores—can reduce total benzodiazepine use and shorten detox duration, while maintaining safety. This strategy suits facilities that can regularly use validated tools like the CIWA-Ar scale to monitor symptoms every 1–2 hours3, 9.
Fixed-schedule protocols involve giving benzodiazepines at set intervals regardless of observed symptoms. This method suits situations where monitoring is less frequent, or when patients have a history of severe withdrawal or cognitive challenges that make symptom reporting unreliable3. While fixed-schedule dosing may slightly increase medication exposure, it’s often safer for high-risk profiles who could deteriorate quickly.
Front-loading involves administering a larger initial dose to rapidly control severe symptoms, followed by tapering. This path makes sense for managing someone with a prior history of seizures or delirium tremens, or when immediate stabilization is critical9.
Yes, navigating these choices can be daunting, especially knowing the risks of both under- and overmedication. But every time you tailor the protocol to your patient’s needs, you’re making a difference. Keep in mind: studies consistently show that appropriate benzodiazepine use prevents severe complications and saves lives9. Next, you’ll see how adjunct medications help manage co-occurring mental health or medical issues.
Adjunct Medications for Co-Occurring Conditions
- Screen for depression, anxiety, and psychotic symptoms.
- Assess for epilepsy, cardiovascular, or liver disease.
- Determine need for anticonvulsants, antipsychotics, or beta blockers.
- Re-evaluate medication compatibility with benzodiazepines.
Addressing co-occurring mental health and medical conditions isn’t just about symptom relief—it’s about protecting your patient’s long-term recovery path. When someone presents with depression or anxiety, selective serotonin reuptake inhibitors (SSRIs) or other antidepressants may be considered, but you’ll want to avoid abrupt initiation or dose changes early in withdrawal due to risk of side effects and diagnostic clarity10.
For psychosis, short-term antipsychotics like haloperidol can manage agitation or hallucinations, especially if symptoms persist beyond the initial withdrawal window3. Opt for this framework when individuals have a known psychiatric history or show severe agitation, paranoia, or persistent hallucinations.
For patients with a seizure history—especially if epileptic—adjunct anticonvulsants like carbamazepine or valproate may be helpful, sometimes reducing overall benzodiazepine requirements3. Beta blockers can stabilize heart rate and blood pressure in those experiencing autonomic hyperactivity, but should be used with caution if underlying cardiac disease is present3.
Prioritize this when multiple medical and psychiatric needs intersect. Every time you tailor adjunct medications to individual co-occurring needs, you’re not just managing withdrawal—you’re giving your patient a better shot at lasting stability. Yes, this can be complicated, but progress happens one careful decision at a time.
Clinical Assessment Tools That Guide Treatment
CIWA-Ar Scale Application in Real-Time
- Assess orientation, tremor, sweating, anxiety, agitation, and hallucinations every 1–2 hours.
- Record and total scores promptly to guide medication dosing.
- Escalate care if scores rise rapidly or symptoms worsen unexpectedly.
The Clinical Institute Withdrawal Assessment for Alcohol, Revised (CIWA-Ar), is a validated tool used to quantify withdrawal severity and direct treatment. By rating ten specific symptoms—including nausea, tremor, sweats, and perceptual disturbances—at regular intervals, you gain a dynamic, objective picture of your patient’s evolving risk.
This hands-on approach allows you to titrate benzodiazepines responsively, minimizing both under-treatment (which can lead to seizures) and over-sedation. This approach is ideal for environments where you have access to staff trained in assessment, and when patients are alert enough to participate.
“Frequent CIWA-Ar scoring every 1–2 hours during the first 48 hours of withdrawal is linked to early detection of deterioration, giving you a real chance to intervene before crises develop.”
In practice, symptom-triggered dosing with CIWA-Ar has been shown to reduce overall medication use, shorten stays, and lower complication rates compared to fixed-schedule regimens3, 9. Yes, the process can feel repetitive and labor-intensive, but every timely score you record is another safeguard for your patient’s safety. Each accurate assessment is a small win—one that builds trust and keeps recovery moving forward.
Determining Appropriate Level of Care
- Review withdrawal severity (CIWA-Ar scores, vital signs).
- Evaluate medical and psychiatric comorbidities.
- Assess social support and risk of self-harm.
- Determine ability for 24-hour monitoring and rapid intervention.
Choosing the right treatment setting is about balancing safety, resources, and the client’s unique needs. Mild withdrawal (CIWA-Ar scores under 8, stable vitals, no history of seizures or delirium tremens) can often be managed in outpatient or low-intensity environments. Consider this route if the individual has strong social support and no significant co-occurring illnesses8.
For moderate-to-severe withdrawal (higher CIWA-Ar scores, history of complications, unstable vitals, or active mental health concerns), inpatient or medically supervised residential care is strongly recommended. These environments provide constant monitoring and immediate access to medical intervention, which is essential for preventing life-threatening events such as seizures or delirium tremens3.
The American Society of Addiction Medicine notes that comprehensive assessment is critical to match the level of care to withdrawal risk factors, ensuring safer and more effective outcomes8. Remember, every step you take to match your client’s risk with the right setting is a step toward a safer recovery. Yes, these decisions can feel high-stakes, but your careful assessment is what makes real progress possible.
Why Detox Alone Produces 8% Success Rates
If you’re coordinating care for someone entering withdrawal, you might be wondering what happens after those first critical days. Here’s the honest truth: detox by itself leads to lasting recovery for only about 8% of people3. That statistic isn’t meant to discourage you—it’s meant to empower you with the knowledge you need to guide your patients toward success.
Here’s what’s really happening: medical detox does exactly what it’s designed to do. It safely stabilizes the body, prevents dangerous complications like seizures or delirium tremens, and gets the individual through the hardest physical part of withdrawal. And that’s huge—it’s the essential first step. But substance use disorders involve more than just physical dependence. The patterns, triggers, and underlying reasons don’t disappear when the substance leaves the system.
This is where comprehensive care makes all the difference. When medical stabilization connects directly to ongoing treatment—therapy, support groups, Medication-Assisted Treatment (MAT), and relapse prevention planning—success rates jump dramatically. Research shows that pairing initial stabilization with continued care can reduce one-year relapse rates from 60–70% down to 35–40%3.
At Pacific Crest Trail Detox, we’ve built our entire approach around this principle. We don’t just help individuals get through the acute phase safely—we walk alongside them into the next phases of recovery, whether that’s our Partial Hospitalization Program (PHP), Intensive Outpatient Program (IOP), standard outpatient services, or DUII court-mandated treatment. Every person deserves a complete roadmap for lasting change. Let’s break down the essential elements that turn short-term safety into long-term success.
Frequently Asked Questions
What’s the typical cost range for medically-supervised alcohol detox programs?
The typical cost range for medically-supervised alcohol detox programs can vary widely depending on the setting, geographic region, and level of medical complexity. While hospital-based programs may incur higher costs due to intensive monitoring and access to emergency services, residential and outpatient detox options are often less expensive. Unfortunately, there is limited standardized public data on exact pricing, as costs are shaped by factors like insurance coverage, medication protocols, and length of stay3. When discussing cost planning, encourage colleagues to consider variables such as staffing ratios, physician oversight, and access to adjunct services. Remember, investing in medical supervision during alcohol detox saves lives and reduces long-term healthcare expenditures by preventing severe complications3.
How do I choose between residential detox and hospital-based programs for moderate withdrawal cases?
For moderate alcohol withdrawal, choosing between residential detox and hospital-based programs comes down to patient safety, available resources, and the likelihood of medical complications. Residential detox offers a supportive, less clinical environment and is suitable for stable patients without high seizure risk or severe medical issues. This path makes sense when 24-hour monitoring and medication management are available, but emergency interventions are rarely needed. Hospital-based programs are preferable if the individual has a history of delirium tremens, unstable vital signs, or significant co-occurring medical conditions, as rapid escalation of care is possible onsite38. Yes, these choices can feel weighty—trust that matching setting to risk factors protects both patient well-being and professional outcomes.
Can telehealth monitoring replace in-person medical supervision during the acute withdrawal phase?
Telehealth monitoring has expanded access to care and is a valuable supplement for ongoing assessment after the acute withdrawal phase. However, during the first 24–72 hours of alcohol detox, in-person medical supervision remains essential for patient safety. Serious complications such as seizures or delirium tremens can develop rapidly, requiring immediate intervention that telehealth alone cannot provide 3. This approach fits well for stable individuals transitioning to outpatient follow-up, but acute withdrawal—especially in moderate-to-severe cases—still demands hands-on, real-time clinical oversight. Yes, adapting to new technology is progress, but your expertise at the bedside is irreplaceable during the highest-risk period.
What insurance coverage barriers should I anticipate when coordinating comprehensive detox-to-treatment transitions?
Anticipate several insurance coverage barriers when coordinating transitions from alcohol detox to ongoing treatment. Common challenges include limited approval for step-down levels of care, preauthorization requirements, and restrictions on the duration or type of therapy covered after detox. Many insurers may authorize medical detox but hesitate to approve extended residential or outpatient services, even when clinically indicated. This can disrupt continuity of care and impact recovery outcomes, especially for individuals needing comprehensive support. Navigating these barriers often means advocating for thorough documentation of medical necessity and collaborating closely with case managers. Yes, tackling insurance hurdles takes patience, but every successful transition is a win for your patient’s long-term stability 3.
How long does the complete medical detox process typically take from admission to discharge?
The complete medical detox process for alcohol withdrawal typically takes 3 to 7 days from admission to discharge, though individual timelines depend on withdrawal severity, co-occurring health conditions, and medication protocols 3. Most acute symptoms emerge within the first 6 to 72 hours, which is when focused medical supervision is essential. Some individuals with complicated withdrawal or underlying medical issues may require a longer stay for stabilization and monitoring. Discharge planning often begins as soon as symptoms are controlled, with transitions to ongoing care coordinated to reduce relapse risk. Every day of safe management is progress worth celebrating 3.
What genetic or biomarker testing can predict individual withdrawal severity and medication response?
Currently, there are no widely validated genetic or biomarker tests that reliably predict an individual’s alcohol withdrawal severity or specific medication response during alcohol detox 23. While research into genetic markers—such as variations in GABA or NMDA receptor genes—is ongoing, most clinical decisions still rely on history, symptom presentation, and standardized assessment tools. Some studies note that certain biomarkers (like carbohydrate-deficient transferrin or liver enzymes) may reflect recent drinking, but they don’t forecast withdrawal risk or treatment outcomes. For now, careful monitoring and personalized medication adjustment remain the gold standard. Yes, it’s natural to hope for more predictive tools, and every advance will help—but your assessment skills are still the most powerful resource.
Building Your Comprehensive Treatment Framework
Recovery isn’t a single event—it’s a journey that needs structure and support at every stage. That’s why building a comprehensive treatment framework matters so much. You need medical supervision during the acute phase to keep patients safe, yes, but they also need what comes after: therapy to understand the patterns behind their use, tools to handle triggers, and a community that gets what they’re going through.

Think of it like building a house. The initial stabilization is the foundation—absolutely essential. But you wouldn’t stop there, right? You need the walls (therapy and counseling), the roof (relapse prevention strategies), and the support beams (ongoing care and community). Each piece strengthens the others. This solution fits perfectly for specialized populations, which is why PCTD offers tailored programs for LGBTQ+ individuals, veterans, professionals, and those with co-occurring mental health disorders.
Here’s what that journey might look like: A patient starts with 5-7 days of medical monitoring where a team tracks vitals and keeps them comfortable. Then they transition to a Partial Hospitalization Program (PHP)—think of it as intensive therapy five days a week where they build new coping skills while still having the security of medical support nearby. As they gain confidence, they step into intensive outpatient care (IOP), attending sessions three times a week while rebuilding their daily routine. Eventually, they move to standard outpatient support, and even after treatment ends, they have access to alumni services and ongoing community connection.
Research shows that people who complete this full continuum of care are significantly more likely to maintain long-term sobriety compared to those who stop after the first week. That’s because lasting recovery isn’t about rushing through steps—it’s about building real, sustainable change one layer at a time. By utilizing tools like ERPHealth software to track statistically significant treatment results, you ensure that every step is measured and effective. You are doing incredible work guiding patients through this continuum. That takes dedication, and you should feel proud of that commitment.
References
- Medication-Assisted Treatment | SAMHSA. https://www.samhsa.gov/medication-assisted-treatment
- Alcohol Research Report | National Institute on Drug Abuse. https://www.nida.nih.gov/publications/research-reports/alcohol
- Alcohol Withdrawal | National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK441974/
- Alcohol Use Disorder: Diagnosis and Treatment | Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/alcohol-use-disorder/diagnosis-treatment/drc-20369250
- NIH Study on Medication-Assisted Treatment for Alcohol Use Disorder. https://www.nih.gov/news-events/news-releases/nih-study-shows-medication-assisted-treatment-alcohol-use-disorder
- Understanding Alcohol Use Disorder | American Psychiatric Association. https://www.psychiatry.org/patients-families/substance-use-disorders/alcohol
- Alcohol and Public Health: FAQs | CDC. https://www.cdc.gov/alcohol/faqs.htm
- Treatment Guidelines | American Society of Addiction Medicine. https://www.asam.org/quality-care/guidelines-and-consensus-documents
- Benzodiazepines and Other Drugs to Manage Acute Withdrawal from Alcohol | PubMed Central. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4084966/
- Alcohol and Mental Health Connection | NAMI. https://www.nami.org/Blogs/NAMI-Blog/Alcohol-and-Mental-Health