Key Takeaways
- Decision Flowchart: Assess clinical complexity → Stabilize acute medical needs → Implement integrated psychological care simultaneously.
- Top 3 Success Factors:
- Integrated Care: Increases sustained recovery to 40-60% (compared to just 8% for detox alone).
- Trauma-Informed Approach: Significantly reduces relapse rates, especially in high-risk populations like veterans and LGBTQ+ individuals.
- Measurable Tracking: Utilizing tools like
ERPHealthsoftware to monitor statistically significant progress in real-time.
- Immediate Next Action: Evaluate your current intake process to ensure you are simultaneously screening for both substance use and underlying mental health disorders.
How Rehabilitation Psychology Shapes Recovery Outcomes
The Brain-Behavior Connection in Addiction
Checklist: Recognizing Brain-Behavior Patterns in Addiction
- Have you noticed persistent cravings or compulsive substance use in your clients, even after negative consequences?
- Do emotional triggers like stress or trauma seem to drive their substance use cycles?
- Is decision-making or impulse control noticeably impaired during periods of active use?
Understanding the brain-behavior connection in rehabilitation psychology can truly empower your practice. You already know that addiction isn’t just a test of willpower—it’s a chronic condition that disrupts the brain circuits involved in reward, motivation, and self-control. Research shows that substance use fundamentally changes the way the brain responds to stress, pleasure, and even basic decision-making. This makes relapse highly likely if only the physical symptoms of withdrawal are addressed4.
Rehabilitation psychology steps in right here, focusing on repairing these disrupted pathways through evidence-based therapy and practical skill-building. Neuroscience has revealed that trauma and chronic stress can prime the brain for addiction by altering emotional regulation and reward processing. For individuals with co-occurring mental health disorders, these changes are even more pronounced, which is why integrated psychological care is absolutely vital.
This approach works best when clients face persistent cravings, struggle with mood instability, or have a history of trauma that fuels their substance use. Addressing the root causes—like shame, low self-esteem, and unresolved trauma—can feel daunting for both you and your clients. Yes, this is challenging work, and that’s okay! Every step toward greater self-awareness helps build new, healthier patterns. Remember, growth isn’t linear; progress may look like fewer impulsive decisions or simply a stronger sense of hope. Each small win is worth celebrating!
Why Medical Detox Alone Falls Short
| Assessment Question | Clinical Indicator | Recommended Action |
|---|---|---|
| Has the individual experienced previous relapses after detox? | Pattern of chronic relapse | Step up to Partial Hospitalization Program (PHP) |
| Are there co-occurring mental health symptoms present? | Anxiety, depression, PTSD | Integrate dual-diagnosis psychiatric support |
| Is there a solid support system or aftercare plan in place? | Lack of safe home environment | Recommend home-like residential aftercare |
| Has the person received psychological counseling during detox? | Medical-only intervention | Introduce Intensive Outpatient Program (IOP) |
Medical detox is a vital first step—especially when managing life-threatening withdrawal from substances like alcohol or benzodiazepines. At Pacific Crest Trail Detox (PCTD), we provide compassionate, non-hospital medical detox to ensure physical safety. However, stopping at detox leaves a massive gap in recovery. While detox addresses the immediate physical dangers, it does not prepare individuals for the emotional, cognitive, and behavioral triggers that drive substance use.
Research shows that when detox is not followed by psychological intervention, only about 8% of people achieve sustained recovery5. That means, without additional support, most individuals are likely to return to use even after their bodies have cleared the substance. Rehabilitation psychology fills this gap by helping people understand the underlying drivers of addiction, such as trauma, shame, and negative thinking patterns.
Consider this method if your clients have a history of relapse, face ongoing mental health challenges, or lack stable support after detox. Psychological support is essential for building new coping skills, repairing relationships, and fostering a sense of hope—all key ingredients for lasting change. Every time you advocate for therapy alongside medical stabilization, you’re helping clients build a true foundation for recovery. You’re doing incredible work guiding them through this!
Core Components of Rehabilitation Psychology
Comprehensive Psychological Assessment
- Screening: Identify co-occurring mental health disorders (depression, anxiety, bipolar disorder, PTSD).
- Evaluation: Assess trauma history and current environmental stressors.
- Cognitive Check: Evaluate cognitive functioning and baseline recovery motivation.
- Barrier Identification: Pinpoint social supports and logistical barriers to change.
A comprehensive psychological assessment is the absolute foundation of effective rehabilitation psychology in addiction care. This process involves gathering detailed information about a person’s mental health, trauma history, emotional regulation skills, and readiness for change. By using standardized tools and clinical interviews, practitioners can clarify diagnoses, spot risk factors for relapse, and uncover strengths to build upon.
For example, a clinician might use structured interviews and validated questionnaires to distinguish between temporary symptoms of substance withdrawal and underlying, chronic depression. This strategy suits organizations that support individuals with complex needs—especially those with both addiction and mental health concerns. According to leading clinical guidelines, integrated assessment helps match people to the right level of care, which drastically improves long-term outcomes7.
The time investment for a thorough assessment typically ranges from 2 to 5 clinical hours per client, often requiring collaborative input from psychologists, social workers, and medical staff. Prioritize this when clients present with ambiguous symptoms, repeated relapse, or when trauma may be an unspoken driver of substance use. Yes, the process can seem demanding, but every piece of insight gained brings you and your clients closer to a tailored care plan that actually fits.
Evidence-Based Therapeutic Interventions
| Client Presentation | Primary Intervention | Expected Time Investment |
|---|---|---|
| Negative thought patterns & triggers | Cognitive-Behavioral Therapy (CBT) | 8–16 weekly sessions |
| Ambivalence about recovery | Motivational Interviewing (MI) | Ongoing throughout early stages |
| Adverse childhood experiences | Trauma-Informed Care (EMDR/CPT) | Long-term engagement (6+ months) |
| Logistical barriers or stigma | Telehealth / Digital Tracking | Flexible scheduling |
When it comes to rehabilitation psychology, the heart of progress lies in evidence-based therapeutic interventions. These are scientifically validated therapies—such as cognitive-behavioral therapy (CBT), motivational interviewing, and trauma-informed care—that consistently help people build new coping skills, manage emotional triggers, and reduce relapse risk. CBT focuses on identifying and reshaping negative thought patterns, while motivational interviewing supports ambivalence and strengthens commitment to recovery.
Trauma-informed approaches acknowledge the impact of past harm and create a safe space for healing, which is especially important for clients with complex histories. Opt for this framework when you’re supporting individuals with both substance use and mental health diagnoses, or when trauma is deeply interwoven with addiction. Research shows that when psychological therapies are included as part of rehabilitation psychology—rather than relying on detox alone—long-term recovery rates increase to 40-60%5.
Resource requirements will vary based on the intervention. CBT or motivational interviewing typically involve weekly sessions over 8–16 weeks, costing roughly $150-$300 per session depending on your region. Trauma-informed programs often require longer engagement and ongoing clinical supervision. While it does take persistence and a dedicated team effort, each successful session is proof that change is possible. Keep encouraging your clients—they are making strides!
Integrated Treatment for Co-Occurring Disorders
Simultaneous vs Sequential Treatment Models
| Clinical Scenario | Recommended Model | Rationale |
|---|---|---|
| Substance use and mental health symptoms are equally severe and intertwined. | Simultaneous (Integrated) | Treating both prevents one from triggering the other. |
| Client has relapsed when one condition was treated before the other. | Simultaneous (Integrated) | Previous sequential failures indicate a need for holistic care. |
| Immediate safety risk from acute withdrawal (e.g., severe alcohol/benzo detox). | Sequential (Stabilize First) | Medical safety must be secured before deep psychological work begins. |
In co-occurring disorders treatment, the choice between simultaneous (integrated) and sequential models is central to client outcomes. Sequential models address one disorder—typically substance use—before moving on to the mental health condition. This path makes sense for situations where acute dangers require urgent medical stabilization, such as severe benzodiazepine or alcohol withdrawal. However, relying solely on sequential care often leaves psychological drivers unaddressed, significantly increasing relapse risk once the client steps down from acute care.
Simultaneous, or integrated, models provide coordinated care for both substance use and mental health disorders at the exact same time. Research consistently finds that integrated care leads to better recovery rates and lower relapse for complex cases. For instance, evidence shows that treating both conditions together reduces symptom severity by up to 60% compared to treating them separately5.
This approach is ideal for individuals whose addiction and mental health symptoms fuel each other. Implementing integrated models typically means a higher initial investment in training, coordination, and team-based care. Yet, the reduction in relapse and hospitalizations translates to long-term savings and a vastly improved quality of life. Yes, shifting your practice to integrated care can be demanding, but every gain in stability for your clients is a massive win worth celebrating.
Trauma-Informed Rehabilitation Approaches
- Do your intake and assessment processes include screening for trauma and adverse childhood experiences?
- Are staff trained in trauma-informed care principles, such as safety, trustworthiness, empowerment, and cultural humility?
- Does your program offer evidence-based trauma therapies alongside addiction treatment?
- Are peer supports and lived experience voices included in your program design?
When supporting clients with both addiction and co-occurring disorders, trauma-informed rehabilitation approaches are absolutely essential. Trauma-informed care means recognizing how experiences of trauma—whether from childhood or later in life—shape both substance use patterns and mental health.
“This perspective shifts the question from ‘What’s wrong with you?’ to ‘What happened to you?’ and aims to build emotional safety, choice, and collaboration throughout treatment.”
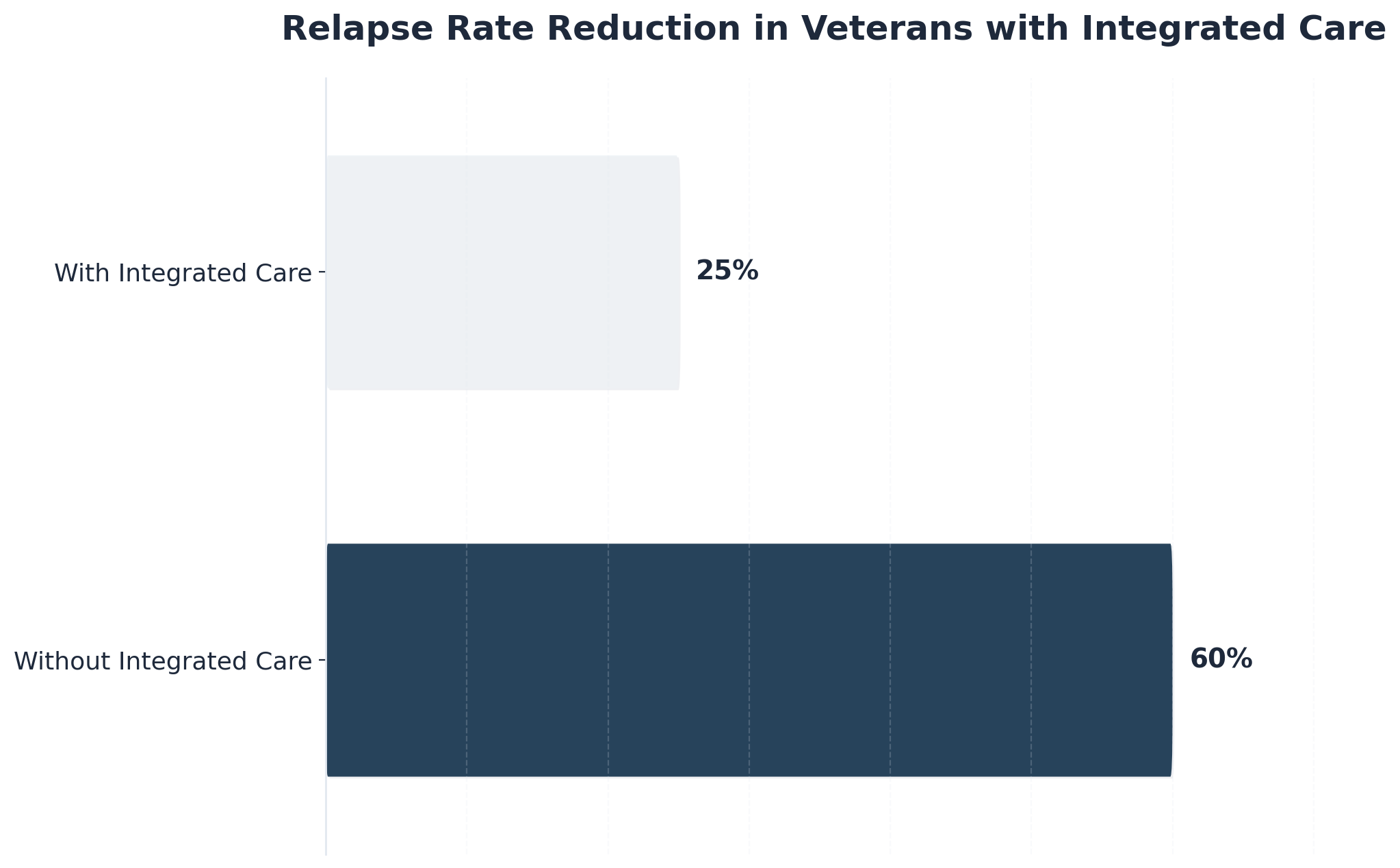
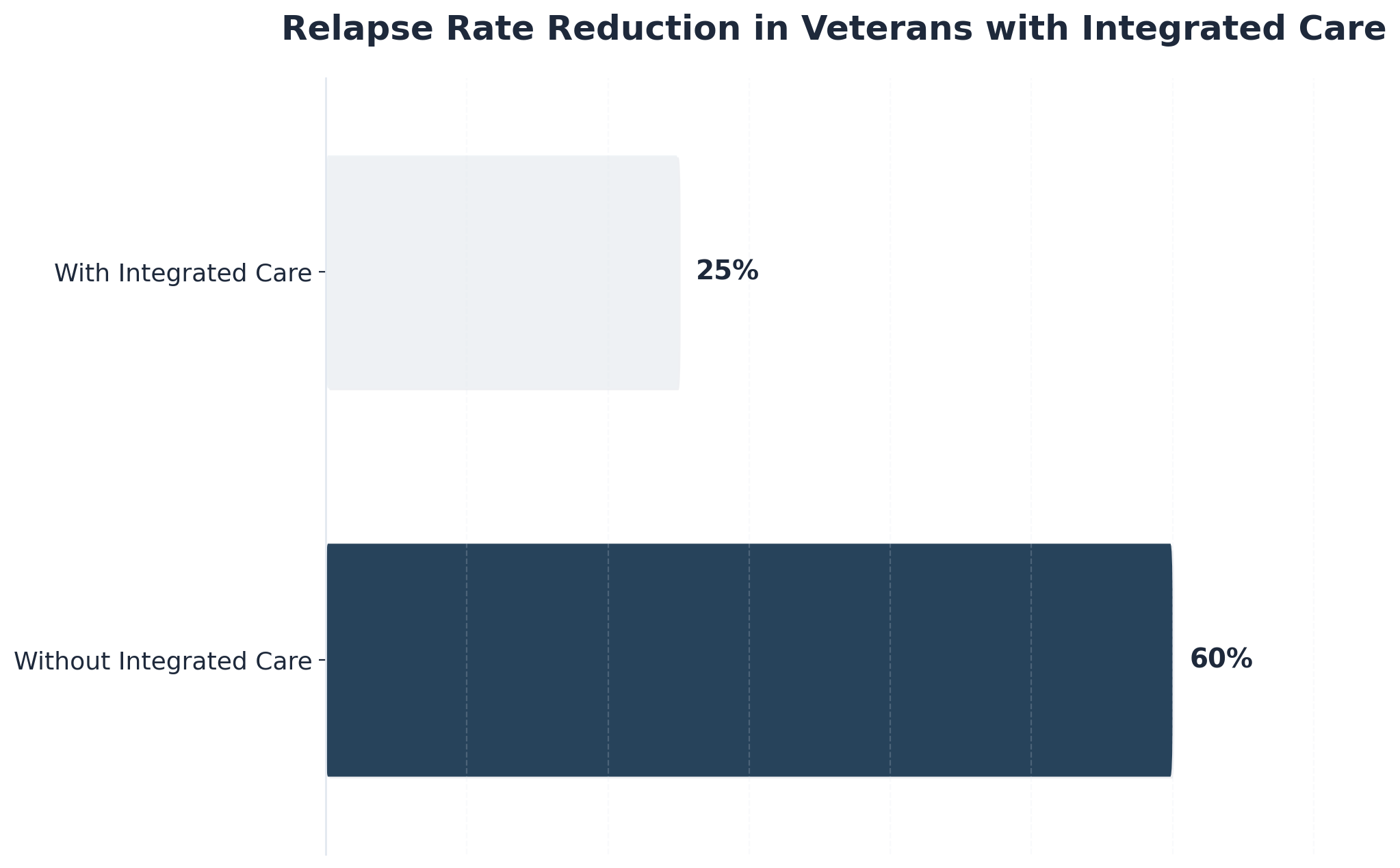
For many, untreated trauma is the underlying driver that makes both addiction and psychiatric symptoms so difficult to manage. This strategy suits organizations working with high-risk populations, such as veterans, LGBTQ+ clients, or individuals with repeated relapse and complex trauma histories. At PCTD, we’ve seen how specialized programs for these populations create the safety needed for true vulnerability and healing.
Research shows that trauma-informed rehabilitation psychology can reduce relapse rates dramatically. For example, veterans receiving integrated trauma and addiction care see relapse rates drop from 60% to 25%6. Implementing these approaches calls for an investment in ongoing staff training, supervision, and dedicated trauma therapy resources. While this may mean higher initial costs, the benefits in client stability are substantial. Navigating trauma in the context of addiction care is tough, but your empathetic guidance helps rewrite their recovery story.
Implementing Personalized Recovery Pathways
When you’re working with patients navigating co-occurring disorders, you know that cookie-cutter treatment plans simply don’t work. Each person walking through your door brings a unique combination of conditions, trauma histories, and life circumstances that require thoughtful, individualized care. At Pacific Crest Trail Detox, we’ve built our entire continuum around this reality—creating personalized recovery pathways that honor the complexity of what you’re seeing in your practice every day.
Building these pathways starts with the comprehensive assessment work you’re already doing. You’re evaluating substance use patterns alongside mental health symptoms, medication histories, previous treatment responses, social support systems, and co-occurring medical conditions. This depth of understanding allows you to design treatment plans that address the whole person rather than isolated symptoms. We track these outcomes through ERPHealth software, which gives us statistically-significant data on what’s actually working—not just clinical impressions, but measurable progress across both addiction and mental health markers.
The sequencing question becomes critical when you’re working with these complex cases. Consider a patient presenting with severe alcohol dependence and major depressive disorder: sometimes you need to stabilize acute withdrawal symptoms in medical detox before you can effectively address the underlying depression. Other times—like with a patient experiencing active suicidal ideation alongside opioid use—managing psychiatric symptoms first creates the foundation needed for successful detox.
At PCTD, we move patients through our continuum (detox → PHP → IOP → outpatient) based on clinical presentation and stability, not arbitrary timelines. A veteran with PTSD and benzodiazepine dependence might need extended PHP support before stepping down, while a professional with high-functioning anxiety and cocaine use might transition more quickly to our specialized intensive outpatient program that accommodates work schedules.
Medication-assisted treatment (MAT) often becomes the cornerstone of these personalized pathways. You’re balancing medications that support recovery from substance use with those managing psychiatric conditions, watching carefully for interactions and adjusting dosages as withdrawal resolves and brain chemistry begins to stabilize. This pharmaceutical choreography requires the ongoing monitoring and frequent adjustments you know are essential during early recovery—it’s delicate work that deserves close attention.
Your therapeutic approach needs to address both conditions simultaneously. Cognitive-behavioral therapy might target addictive thought patterns while also working with depressive cognitions. Dialectical behavior therapy can help with emotion regulation challenges that fuel both substance use and borderline personality symptoms. Trauma-focused approaches recognize that unresolved trauma often underlies both addiction and conditions like PTSD or anxiety disorders. We’ve found this integrated approach particularly effective with our LGBTQ+ patients, who often carry additional layers of trauma and minority stress that impact both conditions.
Building flexibility into these pathways matters tremendously. You’ve seen how recovery rarely follows a straight line, especially with co-occurring disorders creating unexpected challenges. Maybe anxiety spikes during early sobriety, requiring intensified support. Perhaps depressive symptoms emerge as substances are removed and natural mood regulation returns. Effective pathways anticipate these fluctuations and include protocols for adjusting care intensity without disrupting overall progress—stepping someone back up to PHP from IOP isn’t a failure, it’s responsive, compassionate care.
The transitions between care levels deserve your careful attention in treatment planning. Moving from medical detox to partial hospitalization, then to intensive outpatient and standard outpatient care shouldn’t feel like falling off a cliff for your patients. Each transition should be carefully timed based on symptom stability, coping skill development, and environmental readiness—not insurance limitations or facility convenience. We’ve learned that honoring these transitions, even when it means extending care at one level, ultimately produces better long-term outcomes.
Remember, personalization extends beyond clinical interventions. It includes considering your patients’ work schedules, family responsibilities, cultural backgrounds, and personal values. Our specialized programs for veterans, professionals, and LGBTQ+ individuals exist because these populations face unique challenges that generic treatment can’t fully address. Recovery pathways that honor these factors consistently show better engagement and stronger outcomes than those focused solely on clinical protocols—and that’s what we’re all working toward together.
Frequently Asked Questions
How do you determine the right intensity level of psychological intervention for different clients?
Determining the right intensity of psychological intervention starts with a thorough assessment of each client’s clinical complexity, risk factors, and readiness for change. Tools like structured interviews and validated rating scales help clarify whether a client needs standard outpatient therapy, intensive outpatient programming, or partial hospitalization. This strategy suits clients with co-occurring disorders, histories of trauma, or repeated relapse, where higher-intensity support may be crucial for safety and engagement 7. For those with stable living situations and mild symptoms, less intensive interventions often suffice. Remember, rehabilitation psychology is most effective when the level of care matches both current needs and evolving strengths—adjusting as clients grow, struggle, or reach new milestones.
What’s the typical timeline for seeing measurable psychological improvements during rehabilitation?
You’ll usually see measurable psychological improvements during rehabilitation within the first 8–16 weeks of consistent therapy, such as cognitive-behavioral or trauma-informed sessions. Early gains may include improved mood, better impulse control, or stronger coping skills—small but meaningful steps you and your clients can celebrate. This timeline can shift based on the severity of co-occurring disorders, the intensity of intervention, and how regularly clients engage in sessions. Rehabilitation psychology research shows that more comprehensive, sustained interventions (not just detox) are linked to significantly higher rates of lasting improvement—up to 40–60% sustained recovery compared to 8% for detox alone 5.
How do you maintain therapeutic alliance when clients resist psychological work?
Maintaining a strong therapeutic alliance when clients resist psychological work takes patience and flexibility. Start by validating their feelings and exploring what makes psychological work uncomfortable—sometimes, resistance signals fear, past trauma, or a need for more control in the process. Shifting your approach to prioritize safety, choice, and collaboration can make a big difference. Motivational interviewing, for example, helps clients voice their own reasons for change without feeling pressured. This solution fits situations where trust is fragile or past treatment experiences have led to mistrust. Regular check-ins and celebrating small efforts—even showing up—foster hope and engagement over time 7.
What are the cost-benefit considerations when adding rehabilitation psychology to medical-only programs?
When weighing the cost-benefit of adding rehabilitation psychology to medical-only addiction programs, the numbers are incredibly encouraging. While initial investment includes extra staffing, assessment, and therapy time, research shows every $1 spent on integrated psychological care can yield $5–$7 in societal benefits by reducing relapse, improving employment, and lowering criminal justice involvement 9. Only 8% of clients maintain recovery with detox alone, compared to 40–60% when psychological support is included 5. This approach is ideal for organizations aiming to boost long-term outcomes and reduce costly rehospitalizations. Every improved outcome means one more step toward stability and resilience.
How do you adapt rehabilitation psychology approaches for culturally diverse populations?
Adapting rehabilitation psychology for culturally diverse populations means honoring each client’s unique cultural background, beliefs, and values throughout assessment and treatment. Start by building cultural humility—ask open questions about identity and preferences, and invite feedback on what feels respectful and safe. Incorporate culturally relevant practices, such as involving family or community supports, and consider language needs by offering interpreters or bilingual staff when possible. This approach works best when clinicians receive ongoing training in cultural competence and regularly review care plans with a lens of equity and inclusion. Evidence shows that culturally tailored interventions improve engagement and outcomes for diverse clients 10.
What credentials should you look for when hiring rehabilitation psychologists for addiction treatment?
When hiring rehabilitation psychologists for addiction treatment, prioritize candidates with a doctoral degree (PhD or PsyD) in psychology, plus state licensure as a psychologist. Specialized training or certification in addiction psychology, co-occurring disorders, and trauma-informed care is highly valuable. Look for experience with evidence-based therapies, such as cognitive-behavioral therapy and motivational interviewing, as well as demonstrated skills in working with complex cases. Board certification from organizations like the American Board of Professional Psychology in Rehabilitation Psychology can signal advanced expertise 3. This approach is ideal when your program serves individuals with dual diagnoses or trauma histories.
How do you integrate telehealth into rehabilitation psychology without losing treatment effectiveness?
Integrating telehealth into rehabilitation psychology can be highly effective when you focus on maintaining strong therapeutic connection and accountability. Start by using secure video platforms for face-to-face sessions, ensuring privacy and ease of use for clients. Evidence shows that telehealth is particularly useful for follow-up, aftercare, and relapse prevention, especially for clients in rural or underserved areas 4. To keep treatment quality high, combine telehealth with regular goal-setting, digital progress tracking, and flexible scheduling. This approach works best when you check in about technology comfort and provide extra support if clients face barriers. Every successful remote session is proof that recovery support can reach people wherever they are.
Building Your Comprehensive Care Strategy
When developing comprehensive care strategies for patients with co-occurring disorders, the integration of services becomes your most powerful tool. Research consistently shows that detox alone achieves only an 8% success rate without follow-up care—a statistic that underscores why fragmented treatment approaches fail our patients. The professionals who achieve the best outcomes are those who implement truly integrated care pathways from the very first intervention.
A robust continuum model provides the framework many facilities use to ensure seamless transitions. This typically flows from medical detox through medication-assisted treatment, then into partial hospitalization programs, intensive outpatient care, standard outpatient services, and finally structured aftercare. Each phase builds on the previous one, addressing both substance use and mental health conditions simultaneously rather than sequencing them.
Consider this route if you want to maximize patient retention and comfort. At Pacific Crest Trail Detox, this continuum operates within a home-like residential environment rather than a clinical hospital setting—a distinction that can significantly impact patient engagement and comfort during vulnerable early recovery stages. We also accept most insurance (excluding OHP) to ensure this comprehensive care remains accessible to the broader Pacific Northwest region.
As you build treatment plans for your dual diagnosis patients, consider how environmental factors influence outcomes. Evidence-based modalities like cognitive behavioral therapy and dialectical behavior therapy demonstrate stronger results when delivered in settings where patients feel safe enough to engage authentically. Coordinate medical supervision, clinical therapy, and medication management as one unified intervention, not separate services happening to occupy the same timeline.
The goal isn’t simply to treat two conditions—it’s to recognize how they interact and create care strategies that address the whole person. When you implement comprehensive approaches that honor this complexity, you’ll see improved retention, reduced relapse rates, and patients who develop sustainable recovery skills that extend well beyond your direct care. You have the power to make a profound difference in their lives!
References
- Substance Abuse and Mental Health Services Administration (SAMHSA). https://www.samhsa.gov/
- National Center for Biotechnology Information – PubMed. https://www.ncbi.nlm.nih.gov/pubmed/
- American Psychological Association – Addiction Psychology. https://www.apa.org/ed/accreditation
- National Institute on Drug Abuse (NIDA) – NIH. https://www.nida.nih.gov/
- National Institute of Mental Health (NIMH) – NIH. https://www.nimh.nih.gov/
- U.S. Department of Veterans Affairs – Mental Health & Substance Use. https://www.va.gov/HEALTH/
- American Society of Addiction Medicine (ASAM). https://www.americanaddictivesociety.org/
- Cochrane Library – Systematic Reviews of Addiction Interventions. https://www.cochrane.org/
- RAND Corporation – Health & Substance Use Policy Research. https://www.rand.org/
- Centers for Disease Control & Prevention – Mental Health & Substance Use. https://www.cdc.gov/mentalhealth/