Key Takeaways
- Decision Flowchart: Assess client risk level → If high risk (e.g., housing instability), assign a peer specialist within 24 hours → Track engagement using outcome software.
- Top 3 Success Factors: 1) Reducing relapse rates by up to 50% in high-risk groups. 2) Increasing aftercare retention beyond 90 days. 3) Improving housing and employment stability.
- Immediate Next Action: Audit your current post-detox transition plan to ensure clients have a dedicated peer contact before leaving your facility.
How Lived Experience Powers Peer Recovery Support
Welcome! If you are looking to enhance your facility’s aftercare programming, integrating peer recovery support is a transformative step. At Pacific Crest Trail Detox (PCTD) in Milwaukie, Oregon, we understand the challenges you face as industry professionals. We know that medical detox without follow-up care has only an 8% success rate. That is why we emphasize a warm, home-like continuum of care—from sub-acute detox to intensive outpatient programs (IOP)—that truly supports long-term healing.
What Peer Recovery Specialists Bring
| Core Strength | Practical Application in Aftercare |
|---|---|
| Lived Experience | Authentic empathy and credibility from navigating substance use recovery. |
| Hope-Inspiring Relationships | Role modeling and accountability that feels genuine, not clinical. |
| Practical Guidance | Community resource linkage and strategies for early recovery hurdles. |
Peer recovery specialists—sometimes called peer support workers—bring something unique and irreplaceable to aftercare: the wisdom gained from walking their own recovery path. Unlike clinicians, these professionals share lived experience with substance use and recovery, allowing them to offer empathy and hope that feels truly genuine. When someone is facing the daily hurdles of post-treatment life, having a peer who understands the struggle firsthand can make the difference between feeling isolated and feeling seen.
Peer recovery support isn’t just about sharing stories, though. These specialists help people develop strategies for handling triggers, building healthy routines, and staying connected to supportive communities. Their work can include facilitating groups, providing one-on-one mentorship, and helping individuals access everything from housing to job opportunities. This approach is ideal for clients who need encouragement that feels real, not clinical, and practical advice for the unpredictable ups and downs of early recovery.
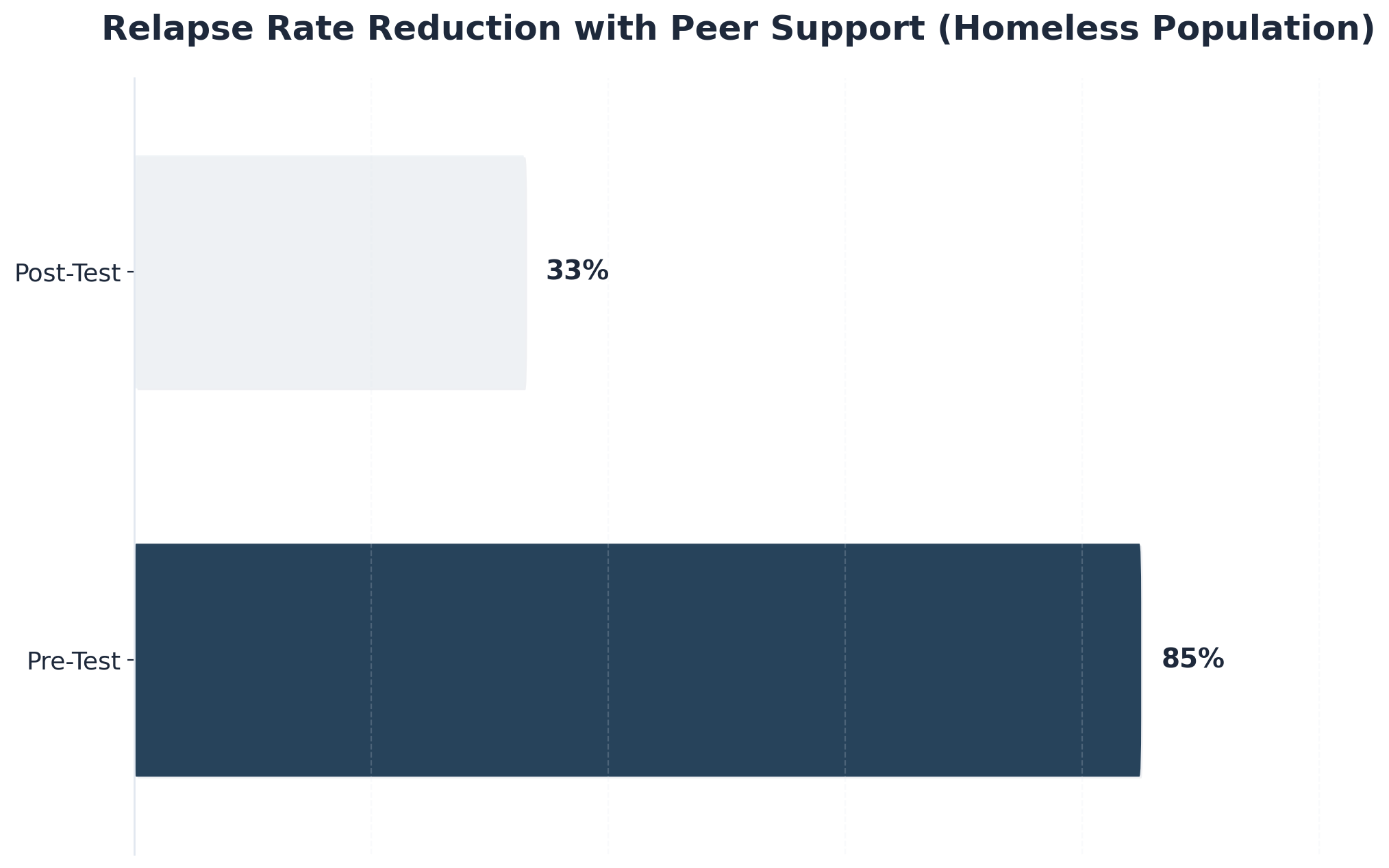
“Studies consistently show that peer recovery support leads to stronger engagement, better retention in aftercare, and lower relapse rates—especially for individuals facing high barriers such as homelessness or social isolation.”
In fact, research found that relapse rates among individuals experiencing homelessness dropped from 85% to 33% after participating in peer support programs3. Every step forward counts, and peer specialists are often the steady hand that helps guide those steps. Next, let’s look at the measurable outcomes and benchmarks that make peer recovery support a trusted approach in aftercare.
Evidence Base and Outcome Benchmarks
Outcome Assessment Tool: Peer Recovery Support Program Benchmarks
- Relapse rate reduction (target: 50%+ decrease in high-risk groups)
- Aftercare retention beyond 90 days
- Improvement in housing stability and employment rates
- Lower acute healthcare use
- Client-reported increases in hope, self-efficacy, and satisfaction
Peer recovery support stands on a solid foundation of research-backed outcomes. Studies show that when peer recovery specialists are integrated into aftercare, measurable improvements follow. For example, research tracking individuals experiencing homelessness found relapse rates dropped from 85% to 33% after participation in peer support programs—an astonishing impact for a group facing some of the toughest barriers in recovery3. This strategy suits organizations that need to move the needle for populations at greatest risk of disengagement or relapse.
Data reveals traditional aftercare without peer involvement achieves only about 8% long-term success1. Systems that include peer recovery support report stronger engagement, higher retention, and increased overall well-being among participants4. Client surveys also highlight greater feelings of hope and belonging, which are essential for sustained recovery. At PCTD, we track these statistically-significant treatment results using ERPHealth software, ensuring our compassionate care is backed by proven data.
Peer recovery support isn’t just a feel-good intervention—it is now recognized by major agencies as an evidence-based practice, and benchmarks like those above can help your team track progress and advocate for resources. Yes, this is challenging, and that’s okay; every step forward counts when it comes to building a program that truly works. Next, we will explore how peer recovery programs bridge the most vulnerable transition period after treatment and what makes this support so critical.
Bridging the Critical Transition Gap
The First 30 Days Vulnerability Window
Quick Assessment: Are Your Clients Supported During the First 30 Days?
- Is there a dedicated peer recovery support contact within 24 hours post-discharge?
- Are clients offered daily or near-daily check-ins for the first two weeks?
- Is support available during evenings and weekends?
- Does your team track engagement and relapse rates in this window?
The first month after leaving detox or residential care is a true pressure point. Research calls this the vulnerability window—when the risk of relapse spikes due to loss of structure, returning triggers, and an overwhelming sense of independence4. Even the most motivated clients can feel the ground shift beneath them. This is where peer recovery support makes an enormous difference: having someone who “gets it” reach out, problem-solve, and just listen can turn a shaky start into a steady foundation.
Consider this route if your organization is seeking to strengthen retention and lower early relapse. Studies show that without strong aftercare, success rates can plummet to just 8%1. Peer recovery support fills the gap between clinical safety nets and real-world challenges, offering encouragement and practical help exactly when it matters most. Whether transitioning into a partial hospitalization program (PHP) or standard outpatient care, every call, text, or meeting in those first thirty days is a win—both for the client and the team supporting them.
Community Integration vs Clinical Care
| Focus Area | When to Prioritize |
|---|---|
| Community Integration | When clients need connection, housing, or employment resources. |
| Clinical Care | For acute psychiatric, medication-assisted treatment (MAT), or medical stabilization. |
| Blended Approach | When clients face overlapping needs or complex barriers. |
Community integration and clinical care each play vital but distinct roles after structured treatment. Community integration focuses on supporting clients as they reconnect with daily life—finding safe housing, building social networks, and accessing practical resources. Peer recovery support excels in this space, helping individuals feel less alone and more capable as they navigate the challenges beyond the walls of a clinic. Opt for this framework when your organization aims to foster long-term recovery through empowerment and belonging.
Clinical care, on the other hand, addresses pressing medical or psychiatric needs with professional oversight and evidence-based therapies. The strongest aftercare programs don’t force a choice. Instead, they weave peer recovery support into clinical pathways, ensuring clients benefit from both worlds. For example, a peer specialist might accompany someone to medical appointments, then help them connect with a local job resource group.
Evidence shows this combination leads to better retention and lower relapse rates than either approach alone4. If your team wants to build a bridge between treatment and independent living, integrating both models can make all the difference. Up next, we will examine proven integration models and what it takes to set peer recovery programs up for success.
Integration Models That Work
Training, Certification, and Competency
Competency Checklist: Building a Qualified Peer Recovery Support Team
- State-approved core training completion (typically 40–80 hours, costing $500–$1,500)
- Certification exam passed and active registry status
- Ongoing education in ethics, boundaries, and trauma-informed care
- Lived experience with sustained personal recovery
- Cultural humility and population-specific insights
Bringing peer recovery support into aftercare starts with ensuring your team is well-trained, certified, and prepared for real-world challenges. Most states now require peer specialists to complete standardized training—usually 40 to 80 hours—covering skills like motivational interviewing, trauma awareness, and ethical practice. This investment of time builds a strong foundation, and many programs also require ongoing continuing education to keep competencies sharp7.
Certification isn’t just a box to tick; it signals credibility and professional readiness. Candidates typically need to pass a written exam and show proof of lived experience in recovery. This path makes sense for your program when you need to build trust with both clients and clinical partners, since certified peers are recognized by Medicaid and other payers as evidence-based providers4.
Ongoing competency means more than technical skills. Prioritize candidates who demonstrate cultural humility and a genuine connection to the populations you serve—whether that’s veterans, LGBTQ+ individuals, or professionals. Yes, mastering these expectations is demanding, but every hour invested in training creates safer, more effective support. Next, you will see how supervision and clear role definition help these trained peers thrive within multidisciplinary teams.
Supervision Frameworks and Role Clarity
Supervision & Role Clarity Tool: 5 Essentials for Effective Peer Recovery Support

- Regular, structured supervision sessions (weekly to biweekly)
- Supervisors trained in the peer support model—not just clinical oversight
- Clear job descriptions outlining peer and non-peer tasks
- Consistent communication channels for feedback and support
- Written policies on ethics, boundaries, and confidentiality
Setting up a strong supervision framework is crucial for the long-term success of any peer recovery support program. Supervision shouldn’t be an afterthought; it is the support system that helps peers navigate ethical challenges, manage boundaries, and avoid burnout. Research shows that models blending both clinical and peer-led supervision—where supervisors understand the unique, non-clinical nature of peer roles—lead to better job satisfaction and lower turnover among peer staff9.
Role clarity is just as important. Ambiguity around what peer specialists can and can’t do often leads to tension with clinical staff, confusion in daily operations, and even legal or ethical risks. Consider this method if your team is expanding or integrating peer recovery support for the first time: define job duties in plain language, emphasize the non-clinical nature of peer work, and reinforce these distinctions during onboarding and ongoing training9. For instance, when logging outcomes in your EHR, staff can simply press Tab to navigate fields and use ICD-10 codes appropriately, ensuring clinical and peer notes remain distinct. Yes, these steps take time, but every effort here protects both your team and your clients.
Overcoming Peer Recovery Support Implementation Barriers
Addressing Stigma and Staff Buy-In
Stigma Checklist: Spotting and Reducing Barriers to Peer Recovery Support
- Are peer support staff introduced as valued team members in meetings?
- Do clinicians receive education on the peer role and its evidence base?
- Is there space for staff to express concerns or ask questions about peer integration?
- Are stories of peer support success shared within your organization?
Addressing stigma toward peer recovery support is an ongoing process, not a one-time fix. Yes, skepticism from some clinical staff is real, especially if they haven’t seen the impact of peer specialists firsthand. Some may question the credibility of lived experience or worry about role boundaries, but research shows that peer support outcomes often match or even surpass those of non-peer professionals1. Building buy-in starts with acknowledging these hesitations openly and using education to bridge the gap.
Hosting joint trainings, inviting peer specialists to share their stories, and highlighting success data can help foster mutual respect. This approach works best when organizations prioritize open communication and transparency, creating opportunities for all staff to learn, reflect, and celebrate small wins together. When teams see that peer recovery support leads to higher engagement and better retention, attitudes begin to shift4. Yes, changing culture is tough—and that’s okay. Every moment of understanding and each shared success moves your program forward.
Compensation and Workforce Retention
Retention & Support Checklist: Building a Sustainable Peer Recovery Workforce
- Review pay equity compared to clinical staff
- Offer paid time off and benefits for full-time roles
- Provide clear career progression pathways
- Implement regular supervision and peer mentorship
- Recognize and celebrate staff achievements
Workforce retention is one of the toughest challenges for peer recovery support programs—and it is closely tied to compensation. Many peer specialists report feeling undervalued when their pay lags well behind other behavioral health workers, which can lead to high turnover and burnout5. Typical hourly wages range from $15 to $22, with annual salaries for full-time positions often falling between $32,000 and $46,000. When peers receive fair compensation, benefits, and recognition, they are not only more likely to stay, but also to thrive and deliver consistent, high-quality support.
Prioritize this when your team is seeing rapid turnover or struggles to fill peer roles. Competitive pay, opportunities for advancement, and acknowledgment of lived experience as a true asset all help build loyalty and a sense of belonging. Yes, budget limitations are real, and that’s okay—small steps like peer mentorship programs or public appreciation can also boost morale and connection. Addressing compensation and career growth isn’t just about fairness. Research shows that when peer recovery support staff feel respected and secure, program outcomes like engagement and retention improve across the board5.
Frequently Asked Questions
What salary range should you budget for peer recovery specialists?
Salary ranges for peer recovery specialists vary widely by region, funding source, and certification requirements. While some states have set minimums, research shows that peer recovery support roles are often paid significantly less than clinical behavioral health workers, contributing to high turnover and job dissatisfaction 5. Typical hourly wages range from $15 to $22, with annual salaries for full-time positions often falling between $32,000 and $46,000 depending on experience, credentials, and local cost of living 5. Programs that invest in equitable compensation, benefits, and clear advancement opportunities are more likely to retain skilled peer specialists and build sustainable support teams. Yes, these investments are challenging, but every dollar spent on fair pay reflects the true value of lived experience in long-term recovery.
How do you handle confidentiality conflicts between peer support and clinical documentation?
Confidentiality conflicts between peer recovery support and clinical documentation are common—and navigating them takes clear policies and teamwork. Peer specialists must honor client privacy, often guided by 42 CFR Part 2 and HIPAA rules, which limit the sharing of personal recovery details with clinical staff unless explicit consent is given. The best approach is to define what information peers document (such as attendance or general support) versus what stays private, and to train all staff on these boundaries. Regular supervision and open communication help resolve gray areas and prevent unintentional breaches 9. Yes, this can feel tricky, but every effort builds trust and keeps your program strong.
Can peer specialists provide support outside traditional business hours?
Yes, peer specialists can and often do provide support outside traditional business hours. This flexibility is a core strength of peer recovery support, especially during evenings and weekends when cravings, loneliness, or crises may feel most intense. Many programs intentionally build after-hours coverage into their models, such as on-call rotations, text-based check-ins, or virtual groups. While not every peer is available 24/7, expanding support beyond 9-to-5 increases engagement and helps clients feel truly supported during vulnerable moments. Research highlights that offering accessible, real-time peer support is linked to better retention and reduced relapse risk in aftercare 4.
How do you measure the ROI of adding peer support to your aftercare program?
Measuring the ROI of peer recovery support involves tracking both financial and client-centered outcomes. Start by monitoring reductions in relapse rates, as programs with peer support have shown drops from 85% to 33% in high-risk populations 3. Next, evaluate improvements in aftercare retention, housing stability, and lowered acute healthcare use. Compare these benchmarks to the costs of program delivery—considering staff salaries, training, and supervision. This approach works best when you also include client-reported increases in hope, self-efficacy, and satisfaction 4. Every positive outcome counts, making the investment in peer recovery support a meaningful long-term strategy.
What’s the typical timeline for building a peer support program from scratch?
Launching a peer recovery support program from the ground up typically takes 3 to 6 months, depending on your organization’s size, resources, and local certification timelines. The process includes developing clear policies, recruiting individuals with lived experience, and ensuring all peer specialists complete state-approved training (usually 40–80 hours) and certification exams 7. Building strong supervision structures and role clarity may add several weeks, especially if you’re new to peer programming. This approach works best when you allocate time for staff buy-in and community partnerships up front. Yes, it’s a big lift, but every milestone means more support for clients at risk of relapse.
Should you hire peers with specific substance use histories to match your client population?
Hiring peers with a specific substance use history to match your client population can be helpful, but it’s not always necessary for effective peer recovery support. What matters most is shared experience of recovery, empathy, and the ability to build trust. Many programs succeed by focusing on core competencies and cultural humility, allowing peer specialists to support a variety of substance use backgrounds 7. This solution fits organizations that serve diverse populations and want flexibility in staffing. If your clients strongly identify with a particular substance, matching can enhance connection—but don’t underestimate the impact of broader lived experience.
How do digital peer support platforms compare to in-person peer services for rural clients?
Digital peer recovery support platforms offer rural clients a lifeline when in-person services are scarce due to distance or lack of transportation. Virtual groups, messaging apps, and video calls can bridge isolation, providing flexible, real-time support. Research highlights that technology-enhanced peer services increase engagement and help reduce relapse risk—especially in areas where face-to-face options are limited 4. This solution fits programs aiming to reach clients in remote locations or those with mobility barriers. However, some clients may miss the deeper connection of in-person interaction, so blending digital and occasional in-person touchpoints often brings the best of both worlds. Every connection—whether online or offline—matters for recovery.
Building Your Aftercare Framework
Effective aftercare frameworks require structured programming that addresses the critical gap between acute treatment and sustained recovery. The data underscores this urgency: detox without follow-up care achieves only an 8% success rate. Building robust aftercare systems means implementing a true continuum of care—from intensive outpatient programs (IOP) through standard outpatient services and ongoing alumni support—that provides the scaffolding clients need during their most vulnerable transition periods.

A comprehensive framework integrates multiple therapeutic modalities with medical oversight. This includes evidence-based individual and group therapy, medication-assisted treatment (MAT) for appropriate candidates, and specialized programming for co-occurring disorders. The structure matters: clients benefit from clearly defined step-down protocols that match intensity to clinical need, whether that’s partial hospitalization, IOP, or traditional outpatient sessions.
Effective programs also incorporate trigger identification protocols, relapse prevention planning, and family therapy components that address the systemic factors influencing long-term outcomes. Implementation requires attention to both clinical and operational elements. Scheduling consistency, alumni services that maintain connection beyond formal treatment, and accessible crisis support systems all contribute to program effectiveness.
The most successful aftercare frameworks combine professional therapeutic intervention with peer support networks, creating redundancy in the recovery infrastructure. When you are developing or refining aftercare programming, focus on measurable outcomes and client engagement metrics—these indicators reveal whether your framework truly supports sustained recovery or simply checks compliance boxes. At Pacific Crest Trail Detox, we are proud to offer specialized programs for specific populations including LGBTQ+ individuals, veterans, and professionals, ensuring everyone finds the compassionate, personalized care they deserve.
References
- Voices of Hope: Substance Use Peer Support in a System of Care. https://pmc.ncbi.nlm.nih.gov/articles/PMC8524681/
- What is the Evidence for Peer Recovery Support Services?. https://dev.recoveryanswers.org/research-post/what-is-the-evidence-for-peer-recovery-support-services/
- Effectiveness of a peer-support community in addiction recovery. https://pubmed.ncbi.nlm.nih.gov/18844242/
- The Impact of Peer-Based Recovery Support Services. https://pmc.ncbi.nlm.nih.gov/articles/PMC12528342/
- Workforce outcomes among substance use peer supports. https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2024.1515264/full
- Barriers and Facilitators to Peer Support Services for Patients. https://pmc.ncbi.nlm.nih.gov/articles/PMC9009995/
- General Peer Support. https://www.samhsa.gov/sites/default/files/programs_campaigns/brss_tacs/peer-support-2017.pdf
- Integrating peer support services into primary care-based OUD treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC9933784/
- The Supervision of Peer Support Specialists. https://peertac.org/wp-content/uploads/2024/06/PTAC-030_Supervision_Guide_06.07.24-3.pdf
- The Power of Peers in Substance Use Recovery. https://casatondemand.org/2025/01/16/the-power-of-peers-in-substance-use-recovery-a-guide-for-behavioral-health-providers/
- PubMed Central. pubmed.ncbi.nlm.nih.gov