
Key Takeaways
- The framing of crossing some invisible line is the wrong question; addiction behaves like a chronic illness, with relapse rates comparable to hypertension and asthma 5.
- Age, body damage, strained family ties, and past relapses are not disqualifiers — many people in long-term recovery got there after multiple attempts paired with medical support 3.
- Detox alone rarely holds, because the 90 days after stopping carry relapse rates near 65–70% for some substances 2; layered care over time is what lowers that risk 7.
- Plan for the danger of unsupervised withdrawal from alcohol or benzodiazepines, which can be life-threatening, and arrange medical supervision plus stable housing and community before stepping down.
The 3 a.m. version of the question
You probably aren’t reading this in a meeting or on a lunch break. You’re reading it because the house is quiet, the phone screen is too bright, and the question keeps circling back: is it too late?
Maybe you’ve tried before. Maybe last week ended in an ER, or a court date, or a conversation with your daughter that you can’t unhear. Maybe you’re sixty-two and you’ve been drinking since you were nineteen and the math feels impossible. Maybe nothing dramatic happened at all, and that’s almost worse, because then it’s just you and the slow, steady knowledge that something has to change.
Here’s what you should know before you read another word: the question you’re asking at 3 a.m. is not the same question a doctor would ask. You’re asking whether you’ve crossed some invisible line. A doctor would ask what’s still working, what hurts, and what we do first. Those have answers. The invisible-line question doesn’t, because that line isn’t real.
This article isn’t going to tell you it’s easy, or that you’ve got this, or that one phone call fixes everything. You’ve heard that before and it didn’t help. What it will do is walk you through what the research actually shows about people in your situation, name the specific fears that are probably keeping you stuck, and describe what the first three days at a place like Pacific Crest Trail Detox in Milwaukie look like in plain language.
Take your time. You can keep reading at your own pace.
What the evidence actually says about ‘too late’
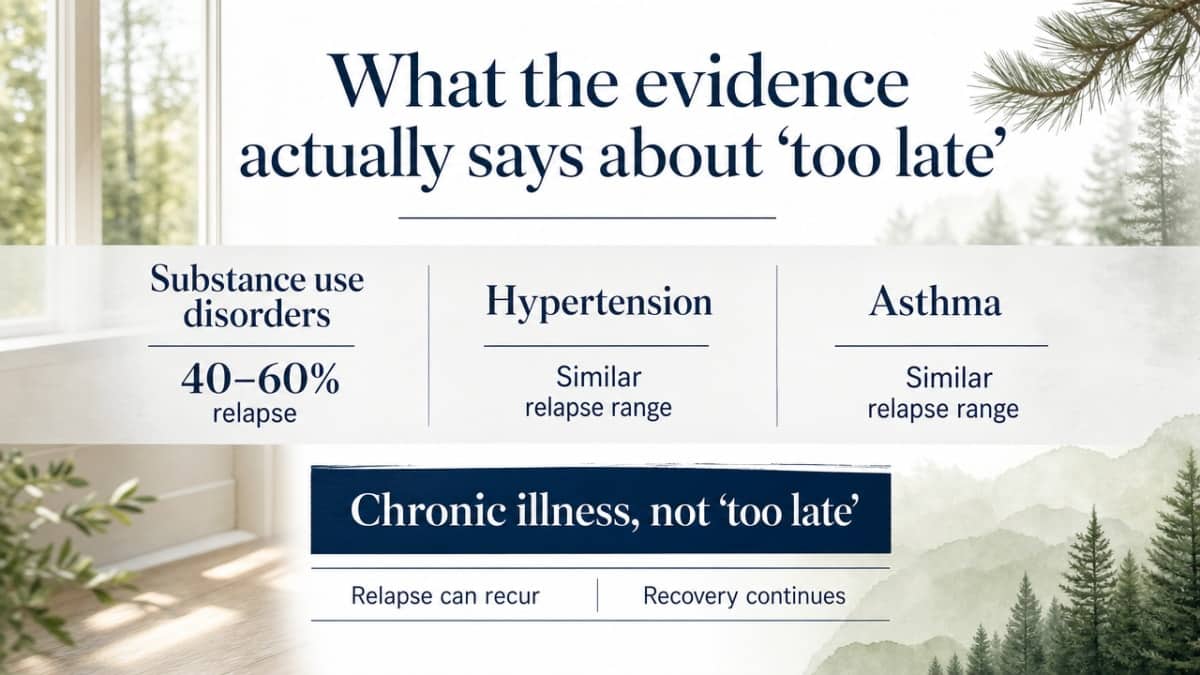
Here is what tends to get lost when you’re awake at 3 a.m.: the people who study addiction for a living don’t talk about “too late.” They talk about chronic illness.
The National Institute on Drug Abuse puts relapse rates for substance use disorders in the 40–60% range, which is roughly the same as relapse rates for hypertension and asthma 5. Nobody tells a person with high blood pressure that their second flare-up means they’re a lost cause. Nobody tells someone with asthma that an attack three years into treatment proves they never really wanted to breathe. Yet that’s exactly the story people tell themselves about addiction, often in their own voice, at night, alone.
The chronic-illness framing isn’t a softening. It’s an accurate description of how the body and brain respond to a substance that’s been part of your chemistry for years. It also changes what “success” looks like. Success isn’t never struggling again. Success is having a plan, a medical team, and people in your corner the next time it gets hard, so the slip stays a slip instead of becoming a season.
The other thing the research keeps showing is that the door doesn’t close with age, or with a long use history, or with multiple past attempts. Studies of people in long-term recovery routinely find that many of them tried, stopped, started, and tried again before something stuck — and that the thing that finally stuck usually involved structured medical support, community, and time, not a sudden burst of willpower 3.
So when you ask, “Is it too late?” the honest answer from the evidence is: that’s not the right question. The right question is, “What’s the first safe step?” That has an answer. And it starts with not coming off alcohol or benzodiazepines on your own, because those two are genuinely dangerous to detox from without medical eyes on you. Everything else — the shame, the math, the years — can be worked with once you’re safe.
The four fears that keep people from calling
‘I’m too old to start over’
If you’re sixty-something and reading this, you might be carrying a quiet version of this thought: the time for big changes was thirty years ago, and now you’re just managing the damage.
That belief is so common it has a name in the research: ageism in addiction care. And it costs people their lives. Nearly 1 million adults aged 65 and older in the United States are living with a substance use disorder right now 9. You are not an outlier. You are part of a very large, very under-treated group of people who were quietly told, sometimes by their own doctors, that this was just how older adults cope.
Here is what the clinical research actually shows: substance use disorders in older adults are treatable conditions when they’re identified and addressed 8. Not “manageable.” Treatable. Trials of naltrexone — a medicine that reduces alcohol cravings — have shown reduced relapse in older adults specifically, even though the wider research on this age group is thinner than it should be 1.
The body at sixty-five is different from the body at twenty-five, and a good detox program plans for that: slower medication tapers, attention to other medications you’re already taking, more time for sleep to come back. At Pacific Crest Trail Detox, that’s the standard, not an accommodation. Starting over at this age isn’t a fantasy. It’s a medical project with a real success rate.
‘I’ve relapsed too many times’
You’ve counted, haven’t you. Three times. Five. The rehab in 2014, the outpatient thing after the DUII, the stretch last spring that lasted four months and felt like proof you could do it before it didn’t.
Each one feels like evidence against you. It isn’t.
The people who study long-term recovery keep finding the same uncomfortable, hopeful pattern: many people who are now stably sober for a decade or more got there after multiple attempts, not on their first try 3. The path wasn’t a straight line for them either. What changed wasn’t their character. What changed was usually some combination of medical support during withdrawal, a real plan for the months after, and people who didn’t disappear when things got hard.
Relapse is also, biologically, most likely in the first ninety days after stopping — some studies put that early relapse rate at 65 to 70 percent for certain substances 2. That’s not a verdict on you. That’s a window the field already knows about, which is exactly why structured aftercare exists. The previous attempts didn’t fail because you’re broken. They likely ended in that ninety-day window without enough support around you. This time, that part can be different.
‘My body is already damaged’
Maybe the bloodwork came back ugly. Maybe your doctor used the word “cirrhosis,” or “early.” Maybe you’ve had a seizure during a past withdrawal, or a heart scare, or you just know — without being told — that something inside you is wearing out.
Here’s the honest part: some damage is permanent. Liver scarring doesn’t always reverse. Nerves take their time. We’re not going to pretend otherwise.
Here’s the rest of it: a lot of damage does heal, slowly, once the substance stops. Liver function often improves. Sleep returns. Blood pressure drops. Cognitive fog lifts in ways that surprise people. And the damage that doesn’t fully heal still gets worse if you keep using and better — or at least stable — if you stop.
‘My family is done with me’
You might be right. They might be done — for now. The voicemails went unanswered. Your sister blocked you. Your kid said something at Thanksgiving that you replay every time it’s quiet.
What you’re feeling is real, and the temptation to use it as proof that there’s no point in trying is enormous. Don’t.
Here’s something worth knowing: in studies of people who built stable, long-term recovery, repaired relationships were almost never the starting point. They were the result. The people in your life who pulled back didn’t do it because you’re unlovable. They did it because they needed to protect themselves from a pattern. The pattern is the thing that can change.
Recovery doesn’t require their permission or their forgiveness to begin. It requires your safety first. The conversations with your family — the careful ones, the messy ones, the ones that might take years — are downstream of you being sober enough to have them. And family therapy, when the time comes and if they’re willing, is something Pacific Crest Trail Detox can help with. But that part is later. The first call is just for you.
Relapse is data, not failure
If you’ve slipped before, you’ve probably treated each one as proof of something permanent about you. A character flaw. A weakness. The thing that means recovery is for other people.
The clinical literature reads it completely differently. Researchers describe relapse as a process, not an event — something with emotional and mental warning signs that show up weeks before the first drink or pill 6. That reframing matters, because a process can be interrupted. A character flaw can’t.
What this means in practice: a slip is information. It tells you what your specific triggers are, what time of day is hardest, which feelings you don’t yet have other tools for, which relationships pull you back toward use. None of that was visible before. Now it is. A good treatment team takes that information seriously and adjusts the plan — different medication, different therapy focus, more support during the hours that keep going sideways — instead of treating you like you’ve failed an exam.
There’s also a timing piece worth holding onto. The most vulnerable window is short and known. Use intensifies the support during that window instead of telling yourself you should be past it.
So if you’ve slipped, here’s what the next 24 hours look like:
- You tell someone.
- You get back to medical care if withdrawal is on the table.
- You let the people in your corner help you read the data instead of grading you on it.
That’s not lowering the bar. That’s how recovery actually works.
Why detox alone is rarely enough
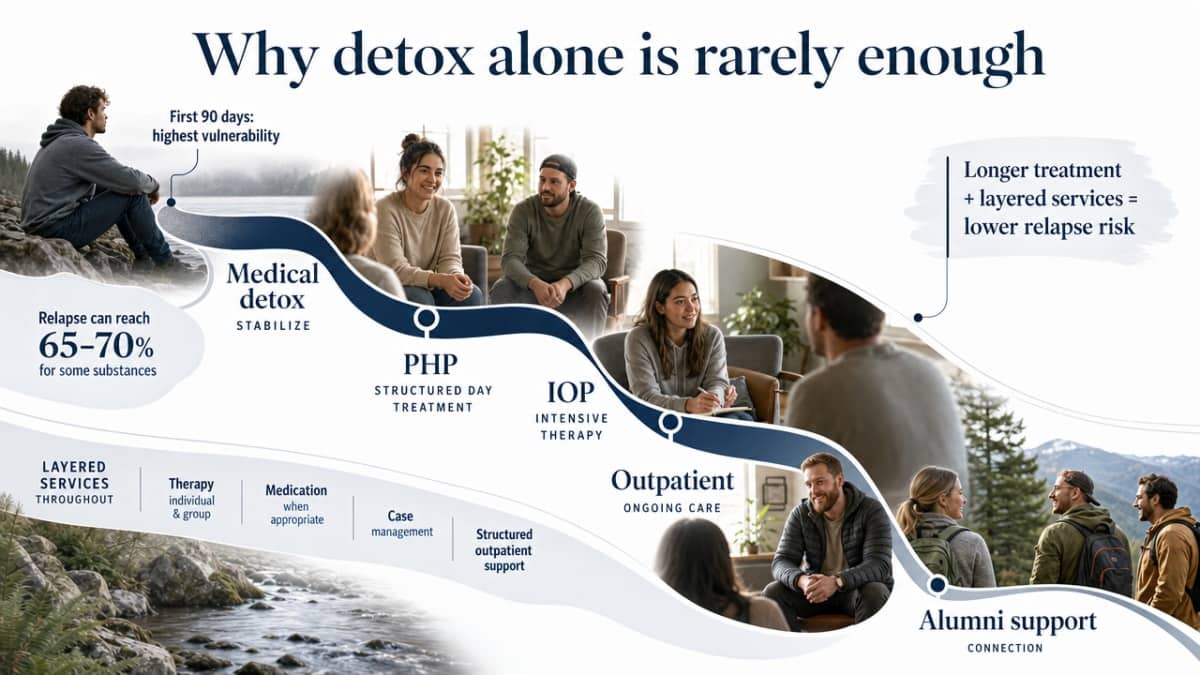
Here’s the part that doesn’t get said often enough at intake: a clean detox, on its own, is not the finish line. It’s the beginning of the window where you’re most vulnerable. Several studies tracking people in the 90 days after they stop using have found relapse rates in the 65 to 70 percent range for certain substances 2. Not because those people lacked grit. Because that window is biologically and emotionally brutal, and willpower is the wrong tool for it.
This is where the chronic-illness framing stops being abstract and starts shaping what you actually need next. The NIDA-funded Drug Addiction Treatment Outcome Study followed thousands of clients across different treatment types and found a consistent pattern: longer stays in treatment, and more services layered on top of detox — therapy, medication when appropriate, case management, structured outpatient days — were tied to lower relapse rates at the 12-month mark 7. The people who did better weren’t the ones with more discipline. They were the ones with more scaffolding around them for longer.
That’s why Pacific Crest Trail Detox isn’t built as a stand-alone three-day stop. It’s built as the first step in a continuum:
- Medical detox to come off safely
- A daytime program you go home from (the partial hospitalization program)
- A less intensive version of that as you stabilize (intensive outpatient)
- Standard outpatient and alumni support — people who stay in your corner after you leave
Each layer is shorter and lighter than the one before it, on purpose. You don’t drop off a cliff after detox. You step down.
If you’ve tried to white-knuckle the months after a detox before, you already know how that ends. It’s not because you weren’t trying. It’s because three days of medical care can’t carry six months of triggers. The point of a continuum is to match the length of the support to the length of the risk.
What the first 72 hours actually look like
One of the reasons “too late” feels so heavy is that the alternative — calling somewhere, packing a bag, walking in — is a black box. You can’t picture it, so you imagine the worst version: fluorescent lights, a clipboard, a stranger asking if you’ve had thoughts of self-harm before you’ve even sat down. Here’s what it actually tends to look like at Pacific Crest Trail Detox, hour by hour.
The first few hours. You arrive at a residential-style house in Milwaukie, not a hospital wing. Someone meets you at the door. A nurse takes your vitals and asks what you’ve been using, how much, and when you last used — the answers don’t surprise anyone, and they’re not written down to be used against you. A doctor reviews your history and decides whether you need medicine to take the edge off withdrawal, especially if alcohol or benzodiazepines like Xanax or Klonopin are in the picture, because those two can be life-threatening to come off without medical eyes on you. The clinical term for that medicine is medication-assisted treatment. The practical version is: you should not feel like you’re being torn apart.
The first night. You have your own room. There’s a bed, a window, a door that closes. The staff checks on you, but you’re not tethered to monitors in a hallway. Sleep may not come easily — that’s normal in the first 24 hours — but the goal is rest, not productivity. Nobody is going to wake you for a 6 a.m. group.
Day two. Withdrawal symptoms usually peak somewhere in this window. Medications are adjusted. You eat real meals at a table with other people who are exactly as nervous as you are. A counselor sits with you, not to dig into your childhood, but to start sketching what comes after detox — because the research is clear that what happens in the weeks after these three days matters as much as the detox itself.
Day three. You’ll start to feel like a person again. Not finished, not fixed — just less like your nervous system is on fire. This is when the conversation shifts toward the next layer of care: the daytime program you’d come back to, the medications you might stay on, the people who’d be in your corner. Trauma-informed care — a clinical way of saying “we assume hard things have happened to you and we don’t make them worse” — runs through all of it 11. You will not be asked to perform gratitude. You’ll be asked what you need next.

Building a life worth staying sober for
A safe place to sleep
One of the quieter truths about recovery is that it’s almost impossible to do from a couch you’re not sure you can stay on next week, or a house where the person you used with still lives, or a car. Stopping the substance is one project. Having somewhere predictable to wake up is another, and the second one carries the first.
Research from Johns Hopkins on stable housing puts it plainly: a safe place to live gives people the stability to focus on the rest of their health, including recovery from substance use 13. It’s not a luxury layered on top of treatment. It’s part of what makes treatment work. When your nervous system isn’t bracing for where you’ll sleep, it has room to do the slower work of healing.
For some people leaving detox, home is fine. For others, the honest answer is that going back to the same address means going back to the same use within a week. Part of what the team at Pacific Crest Trail Detox helps you sort out before you leave is which one you are, and what a workable next address looks like if home isn’t it.
People who stay in your corner
You cannot do this alone. Not because you’re weak — because nobody does. The people who are ten and twenty years into stable recovery almost universally point to the same thing when asked what made it stick: other people. Social support, peer connection, a community of some kind that didn’t disappear when things got boring or hard 3.
That community looks different for different people. For some, it’s Alcoholics Anonymous or another 12-step group, which the research consistently shows is an effective, free, widely available source of long-term support for alcohol use disorder 4. For others, it’s a non-12-step group, a SMART Recovery meeting, or a faith community. Reviews of mutual help groups for drug use disorders find that engagement — pretty much regardless of the specific flavor — is tied to better outcomes 12.
What Pacific Crest Trail Detox adds to that is its alumni program: people who came through the same doors you did, sometimes years ago, who stay reachable. Not as cheerleaders. As witnesses. They’ve already had the bad Tuesday you’re going to have, and they picked up the phone.
Purpose, not just abstinence
Here’s something nobody tells you in the first week: not drinking, by itself, is not a life. It’s a clearing. What you put in that clearing is the actual project, and it’s the part that decides whether sobriety feels like punishment or like coming home.
The Harvard physician who wrote openly about being eleven years into recovery from opiate addiction made the same point from the other side: people don’t just stop using and white-knuckle forever. They build full lives — work that matters to them, relationships that aren’t transactional, mornings they want to wake up for 10. The vulnerability doesn’t vanish. The life around it gets bigger than it.
You don’t have to know what your purpose is on day four. Most people don’t. What you need is a clearing, the medical support to keep it, and time. The rest — the work, the people, the reasons — tends to show up when you give it room to.
How to make the call today
You can make this small. Smaller than the decision feels right now.
The call to Pacific Crest Trail Detox isn’t a commitment to the next year of your life. It’s a conversation. Someone picks up, asks a few questions about what you’ve been using and when you last used, and tells you honestly whether you need to come in today, tomorrow, or whether a different level of care fits better. If alcohol or benzodiazepines like Xanax or Klonopin are part of the picture, they will lean toward today, because those withdrawals are the dangerous ones.
You don’t have to have your insurance card in front of you. You don’t have to have told your family yet. You don’t have to know what to say. “I think I need help coming off ___” is enough of a sentence. The person on the other end has heard it before, from people in exactly your situation, and they will take it from there.
Check What Coverage You Have for Detox Now
See in minutes if your insurance supports your next step toward recovery.
Frequently Asked Questions
Am I too old for detox and treatment to actually work?
No. Clinical reviews describe substance use disorders in older adults as treatable conditions when they’re identified, and medications like naltrexone have shown real benefit for older adults with alcohol use disorder 8. A good detox program adjusts for slower tapers, other medications you’re on, and recovery time. Your age is information your medical team uses to plan well, not a reason to stop trying.
I’ve relapsed several times before. Does that mean recovery won’t stick this time?
No. Many people in stable long-term recovery got there after several attempts, not on their first try 3. Past relapses usually point to what was missing — medical support during withdrawal, structured care in the months after, people who stayed reachable — rather than something wrong with you. The previous tries weren’t wasted. They told you what this attempt needs to include.
How do I know if I need medical detox instead of quitting at home?
If you’ve been drinking heavily for a long time, or using benzodiazepines like Xanax, Klonopin, or Ativan, do not stop on your own. Those two withdrawals can cause seizures and can be life-threatening. Opioid withdrawal is rarely deadly but is brutal enough that most people relapse without medical help. When in doubt, call and let a clinician decide. The phone call itself doesn’t commit you to anything.
What happens after detox ends? Is a few days really enough?
A few days of detox handles the physical part of coming off safely. It doesn’t, by itself, carry you through the months that follow, which is when most relapses happen. NIDA-funded research found that longer treatment and more layered services produced lower relapse rates at one year 7. That’s why Pacific Crest Trail Detox moves you into daytime programs, outpatient care, and alumni support after detox — not instead of it.
How do I bring this up with a family member who may have given up on me?
You don’t have to fix the relationship before you start. Studies of people in long-term recovery show that repaired relationships tend to be a result of recovery, not a prerequisite 3. A short, honest message — “I’m getting help. I’m not asking you for anything right now” — is often enough. Family therapy is available later, when you’re stable and they’re ready. Start with your safety first.
What should I expect when I call Pacific Crest Trail Detox?
Someone picks up. They’ll ask what you’ve been using, how much, and when you last used. Nothing you say will shock them. They’ll talk through whether you need to come in today or whether another level of care fits better, and what your insurance covers (PCTD accepts most plans, excluding OHP). You don’t need paperwork ready. “I think I need help” is a complete sentence.
References
- Substance use disorders among older adults: A review of epidemiology and treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC6757194/
- New Findings on Biological Factors Predicting Addiction Relapse. https://pmc.ncbi.nlm.nih.gov/articles/PMC3674771/
- Pathways to Long-Term Recovery: A Preliminary Investigation. https://pmc.ncbi.nlm.nih.gov/articles/PMC1852519/
- Comparison of 12-step Groups to Mutual Help Alternatives for AUD. https://pmc.ncbi.nlm.nih.gov/articles/PMC5193234/
- Treatment and Recovery | National Institute on Drug Abuse (NIDA). https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
- Relapse Prevention and the Five Rules of Recovery. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553654/
- NIDA-Drug Addiction Treatment Outcome Study (DATOS) Relapse as a function of treatment services and duration. https://pmc.ncbi.nlm.nih.gov/articles/PMC4455957/
- Substance Abuse Among Older Adults. https://pmc.ncbi.nlm.nih.gov/articles/PMC4146436/
- Substance Use in Older Adults DrugFacts. https://nida.nih.gov/publications/drugfacts/substance-use-in-older-adults-drugfacts
- Does addiction last a lifetime? – Harvard Health. https://www.health.harvard.edu/blog/does-addiction-last-a-lifetime-2018100814962
- Study protocol: implementing and evaluating a trauma-informed intervention for patients with substance use disorders in acute care settings. https://pmc.ncbi.nlm.nih.gov/articles/PMC10572352/
- Effectiveness of Mutual Help Groups for Illicit Drug Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12360454/
- How Stable Housing Supports Recovery from Substance Use Disorders. https://opioidprinciples.jhsph.edu/how-stable-housing-supports-recovery-from-substance-use-disorders/


