Key Takeaways
Why Benzodiazepines Require a Careful Detox Approach
If you are reading this after a difficult night, please know you are not alone. Seeking help to stop these medications is a sign of strength, not failure.
Benzodiazepines, such as Xanax, Klonopin, Ativan, and Valium, are unique among substances in how the body adapts to them. While quitting alcohol abruptly can be dangerous and opioid withdrawal is intensely difficult, stopping benzodiazepines suddenly after prolonged use can lead to seizures and life-threatening withdrawal symptoms in physically dependent individuals. This is why every major clinical guideline, including the upcoming 2025 joint guideline from ten medical societies, explicitly states that these medications should not be stopped abruptly in dependent patients.3,9
The idea of “just powering through” does not apply here. Your nervous system adapts to the medication, and removing it too quickly leaves your brain without the calming effect it has come to rely on. The solution is not willpower, but a slow, doctor-supervised dose reduction, with professional oversight, sleep support, and a clear plan for challenging moments.
Developing dependence is not a personal failing. Many individuals were prescribed these drugs for anxiety, panic, or insomnia and followed their doctor’s instructions precisely. What is needed now is a treatment approach that respects your body’s biological responses, focusing on a supportive, monitored process rather than a harsh, isolated attempt. This guide will outline what that process looks like, particularly in the Portland area.
Physical Dependence vs. Addiction: Understanding the Distinction
It is crucial to understand that if your body requires a benzodiazepine to function normally, this is physical dependence. This is not, by itself, addiction.
The 2025 joint guideline from ten medical societies clarifies this point: physical dependence is a common and expected outcome of taking a benzodiazepine for any significant period. Clinicians should not automatically assume that a patient with physical dependence has a substance use disorder. It is simply your biology adapting to a medication you have been taking.9
A substance use disorder involves different characteristics, such as a loss of control over use, taking more than intended, continued use despite negative consequences, and intense cravings that dominate daily life. While some individuals may develop both dependence and a use disorder, many experience only physical dependence. Recognizing this distinction is the first step toward appropriate treatment.
This understanding is vital because it reframes the treatment journey. If you were prescribed Klonopin for panic attacks five years ago and used it as directed, you are not entering treatment to confess a moral failing. You are seeking to safely discontinue a medication your body has adapted to, with the support of professionals who understand the pharmacology involved.
This perspective also shapes what effective care entails. It means collaborative decision-making with your clinician, rather than a prescriptive approach. It involves a personalized tapering plan based on your specific dose, history, and how your body responds, not a generic protocol. Furthermore, your support team should be able to differentiate between a craving and a withdrawal symptom, as misinterpreting these can lead to less effective care.2
You deserve to maintain your dignity throughout this process. This is not just a comforting phrase; it is a fundamental principle of clinical care.
The Seizure Risk Guiding Clinical Decisions
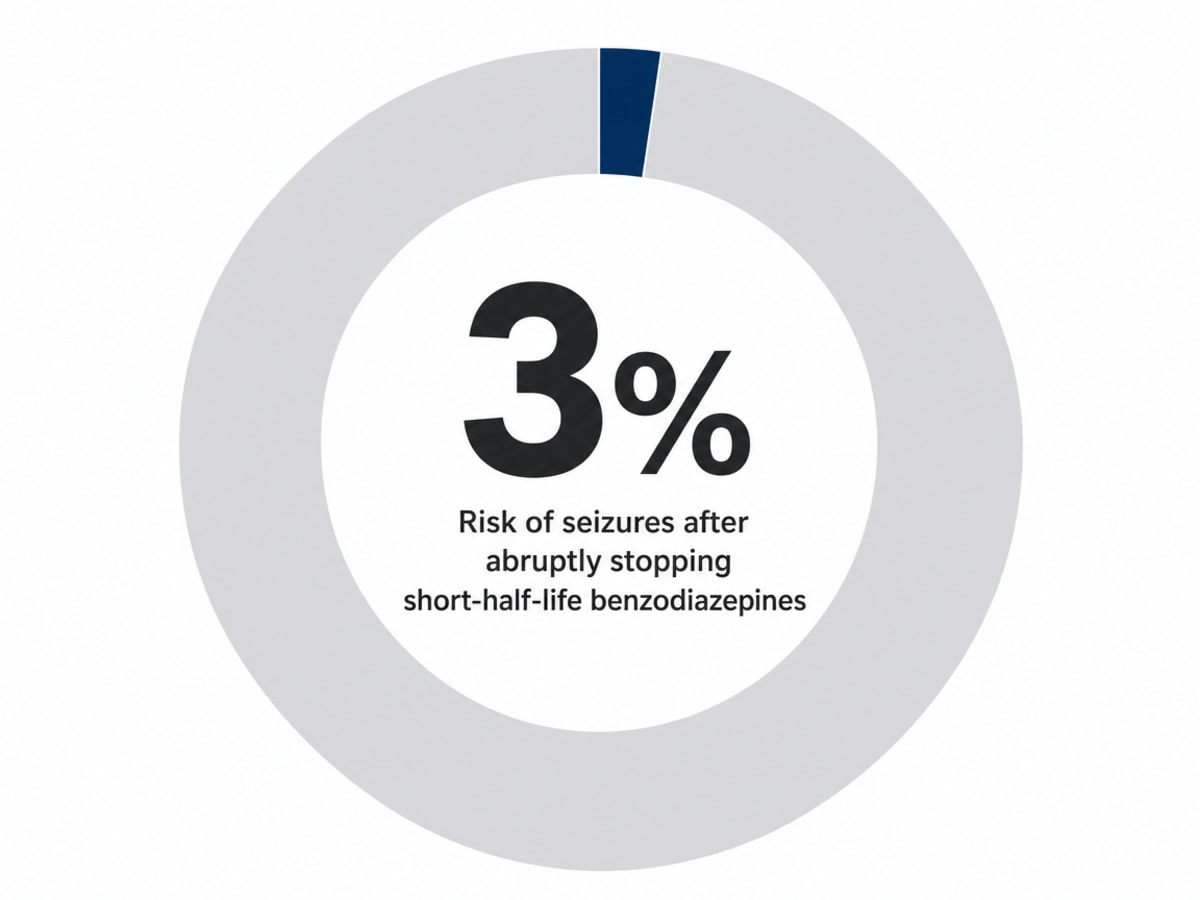
A critical fact to understand is that studies show approximately 3% of individuals who abruptly stopped short-half-life benzodiazepines, like Xanax and Ativan, experienced seizures during withdrawal. While this percentage may seem small, it is significant enough to influence every decision a responsible clinician makes regarding your care.10
A seizure is a serious medical event that can occur unexpectedly and lead to severe injury or further complications, potentially requiring emergency hospitalization instead of a controlled taper. Individuals most at risk are often those who attempt to stop on their own, such as long-term users of short-acting benzos who have run out of medication, are between prescribers, or decide to quit cold turkey.
Consider the contrast: an abrupt stop carries a 3% seizure rate in the studied population, whereas a guideline-paced taper involves small, gradual reductions over weeks, with continuous monitoring by a clinician. This difference represents the gap between a potential medical emergency and a structured path to recovery.9,10
Therefore, your taper should not be rushed due to impatience or a rigid calendar. If symptoms intensify, the pace should slow. As you stabilize, the next reduction can occur. The plan adapts to your nervous system’s needs, offering a compassionate approach even when the process feels challenging.
Understanding a Medically Supervised Taper
Many people envision detox as a quick, intense event. However, for benzodiazepines, this perception is inaccurate and can be dangerous. A true taper is a slow, deliberate process, more akin to carefully descending a staircase than jumping off a cliff. You begin at your current dose, achieve medical stability, and then, and only then, does the gradual reduction commence. The goal is not to endure extreme discomfort but to allow your nervous system to gradually re-learn how to function with less medication, one small step at a time.
The 2025 joint guideline describes this as a collaborative effort between you and your clinician, jointly deciding the pace, monitoring your body’s responses, and adjusting the plan based on your symptoms. There is no one-size-fits-all protocol because every patient is unique. An individual taking 0.5 mg of Klonopin for eight months will have a different starting point and timeline than someone on 6 mg of Xanax for fifteen years.9
The 5–10% Rule and Patient-Specific Pacing
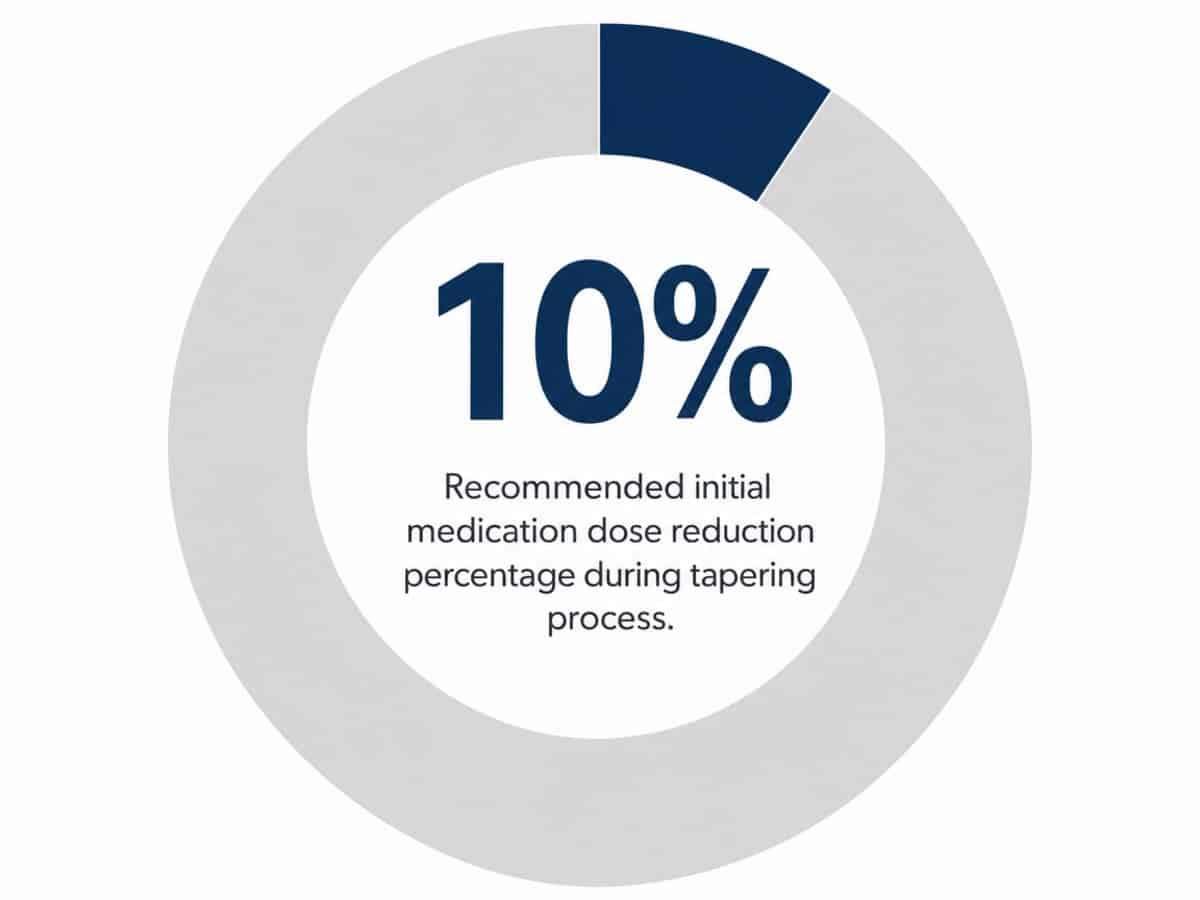
The accepted standard involves initial dose reductions of approximately 5 to 10% at a time, with the overall rate generally not exceeding 25% every two weeks. This is a critical point often misunderstood by those attempting to taper independently: reductions are gradual, often slower than a quarter of your dose every two weeks.9
For individuals on higher doses long-term, a complete taper can take many months, sometimes exceeding a year. This extended duration is part of the plan, not a sign of failure. Your clinician will monitor for changes in sleep, anxiety levels, sensory symptoms, and any indications that your nervous system requires a pause before the next reduction.9
“Patient-specific” means that if a 10% reduction is well-tolerated for a couple of cycles, that pace can continue. However, if a reduction causes significant distress, such as severe sleep disruption or panic, the plan will be adjusted—either paused, reversed, or modified to smaller cuts spaced further apart. The 2025 guideline explicitly states that tapering should be customized to your individual response, not dictated by a calendar. Your honest feedback is the most valuable information for guiding the process.2
Initial Stabilization and Support
The first two weeks are foundational. Often, this period focuses on stabilization rather than active dose reduction. This might involve switching from a short-acting benzodiazepine like Xanax to a longer-acting one, which provides more consistent blood levels and reduces fluctuations between doses, often significantly reducing initial discomfort.
Sleep disturbances are a common challenge for those attempting to withdraw alone. A clinical setting can provide comprehensive sleep support without simply adding more sedatives. This includes non-benzodiazepine sleep aids, establishing a consistent sleep schedule, promoting low-stimulation evenings, and having staff available for support during nighttime anxiety. The 2025 guideline also emphasizes integrating psychosocial support, such as counseling, group therapy, and practical anxiety management skills, alongside the medical taper. The medication manages the pharmacology, while the therapeutic program supports the process of relearning coping mechanisms.9
Choosing the Right Setting: Residential, Outpatient, or Hospital
There are three primary environments for benzodiazepine detox: hospitals, outpatient clinics, and residential programs. The most suitable option depends on your current dose, medical history, and overall life stability.9
- A hospital setting is appropriate for acute crises, such as active seizures, suicidal ideation, or withdrawal from multiple substances simultaneously. However, hospitals are designed for short-term, acute care, not the prolonged, gradual process required for a benzodiazepine taper, which can span weeks to months. While initial stabilization occurs in a hospital, the extended tapering process typically needs to continue elsewhere. The success of the taper often hinges on the quality of this subsequent care.
- Outpatient care, which involves seeing a prescriber and therapist while living at home, can be effective for some individuals, particularly those on lower doses with a stable home environment and no co-occurring substance use issues. The 2025 joint guideline supports lower levels of care when clinically appropriate. However, for many, the home environment might also be associated with past struggles, making a change of scenery beneficial.
- Residential, home-like detox programs often provide an ideal middle ground for benzodiazepine dependence. They offer medical supervision during the most challenging initial phases—stabilization, medication conversion, and the first dose reductions—without the sterile, high-tech atmosphere of an inpatient ward. These settings are designed to feel more like a comfortable home, with private rooms, common areas, shared meals, and natural light. This environment is crucial because benzodiazepine recovery involves helping your nervous system learn to feel safe and regulated without medication. A calm, supportive atmosphere facilitates this process more effectively than a clinical, institutional one.
Residential programs also address the social and therapeutic aspects of recovery. The 2025 guideline explicitly recommends pairing medical tapering with psychosocial support, including counseling, group sessions, and opportunities to practice anxiety management skills. Living in a residential setting with others undergoing similar experiences, and with clinicians readily available, provides a robust support system. You are not left to process difficult group sessions alone; instead, you have immediate access to support within the facility.2
Often, individuals transition through these levels of care: starting with residential for the acute phase, then moving to a partial-day program, followed by intensive outpatient care, and finally weekly outpatient therapy and aftercare. The tapering process itself frequently continues across all these stages.
Understanding Protracted Withdrawal Symptoms (BIND)
It is important to be aware that some individuals experience symptoms that persist long after the acute withdrawal period. This phenomenon is known as Benzodiazepine-Induced Neurological Dysfunction, or BIND. Recent research has begun to quantify these experiences.
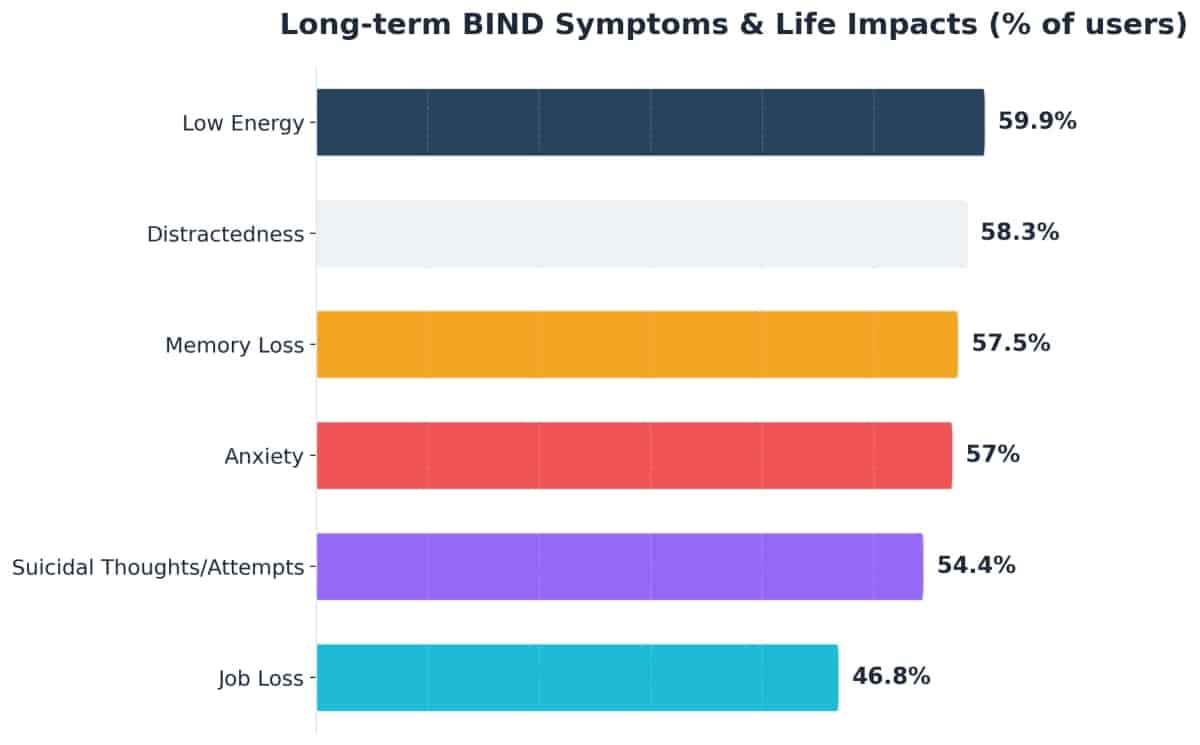
A 2023 self-reported survey of 1,207 benzodiazepine users indicated that over half reported symptoms lasting a year or longer after stopping: 59.9% experienced low energy, 58.3% distractedness, 57.5% memory loss, and 57.0% anxiety. Beyond these symptoms, 54.4% reported suicidal thoughts or attempts linked to benzo use or withdrawal, and 46.8% reported job loss. It is important to note that this was a self-selected internet survey of individuals already concerned about their benzodiazepine use, not a representative sample of all patients. Those who recover smoothly are less likely to participate in such surveys.1
The reason to share this information is to empower you with knowledge. The most challenging aspect of BIND can be feeling isolated and unaware that others share similar experiences. Knowing about BIND serves two key purposes. First, it encourages a slower, more gentle taper from the outset, as current data suggests careful pacing may reduce the likelihood of protracted symptoms. Second, it provides language and context for any lingering symptoms you might experience months later, helping you understand that a flare of anxiety or cognitive fog at month seven could be your nervous system still recalibrating, rather than a sign of personal failure.9
While not everyone experiences the most severe forms of BIND, some do. A comprehensive program acknowledges both possibilities, planning for a paced taper initially and ensuring robust follow-up care, rather than assuming recovery ends the day the last dose is taken.
Portland’s Unique Approach to Benzodiazepine Treatment
While benzodiazepine taper programs exist in many cities, Portland offers a distinct advantage due to its local clinical environment and the contributions of local researchers to national standards.
Historically, Oregon has seen significant prescribing rates for benzodiazepines and opioids. In 2012, Oregon pharmacies dispensed benzodiazepines at a rate of 106.5 prescriptions per 1,000 residents, and 47% of Oregonians received an opioid prescription in the same year, with an unintentional benzodiazepine overdose death rate of 0.6 per 100,000. Although prescribing patterns have evolved, this history means that many households in the Portland metro area have long been familiar with both types of medications. This context underscores why a careful, supervised taper, rather than an abrupt cessation, is the appropriate standard of care locally.4
Oregon’s medical community has actively addressed this issue. In 2022, the state’s Mental Health Clinical Advisory Group published four practical resources specifically for benzodiazepine care, including a tapering guide with example schedules, a tool for deprescribing conversations, and a patient-focused benzodiazepine guide. These resources demonstrate a commitment to safe prescribing and tapering practices within the state’s clinical guidelines.7
Furthermore, Portland plays a quieter but significant role in the national conversation around benzodiazepine care. The Alliance for Benzodiazepine Best Practices, which contributed to the 2023 BIND survey research, includes Portland-based investigators. This means that choosing supervised care in Portland connects you to a region where leading experts on long-term benzodiazepine effects are actively working and contributing to best practices. This is a tangible reason why the local standard of care is aligned with the most current understanding of benzodiazepine withdrawal and recovery.1
Post-Acute Phase: Outpatient Care, Therapy, and Relapse Prevention
Completing the initial, more intensive phase of a taper is not the end of treatment; it is often closer to the halfway point. Your dose may still be decreasing, sleep patterns might still be irregular, and your nervous system will continue its long recalibration. The setting may change, but the ongoing work remains essential.
Many individuals transition from residential care to a partial-day program, which involves structured therapy and medical check-ins several days a week. This is often followed by an intensive outpatient schedule, and then standard weekly therapy. The tapering process itself frequently continues through these different levels of care, with reductions becoming smaller and slower as the dose decreases. The final 10% of a benzodiazepine taper can often be the most challenging, highlighting the importance of continued clinical support during this phase.9
Therapy is where you develop the skills that the medication previously provided. This includes cognitive behavioral therapy for anxiety and insomnia, group sessions with peers undergoing similar experiences, and family or couples therapy if relationships have been affected. The 2025 guideline identifies psychosocial support as a fundamental component of tapering, not merely an optional add-on.2
Relapse prevention in this context is not about sheer willpower. It involves learning to distinguish between a returning symptom and a craving, having a prescriber you can contact before refilling an old prescription, and developing a plan for managing potential BIND-like symptoms that may emerge months later. The journey continues, but with different, sustained support systems in place.1
Navigating Treatment Costs and Key Questions Before Admission
The question of cost is often a primary concern for family members and can be a source of apprehension for the individual seeking treatment. Both reactions are understandable. Here is a straightforward overview.
Most private insurance plans, including employer-sponsored, marketplace, and many union plans, typically cover medically supervised detox and subsequent levels of care. However, coverage details vary significantly, encompassing deductibles, in-network status, prior authorization requirements, and the number of approved residential days. The Oregon Health Plan (Medicaid) operates differently, and not all private detox facilities accept it. It is crucial to confirm coverage details before admission.
Before committing to any program, consider asking the following questions:
– Is there a prescriber on staff specifically experienced in managing benzodiazepine tapers, and do your protocols align with the 2025 joint guideline’s recommended pace?- How will my taper be managed after I complete residential care, and who will oversee it?- What psychosocial support services are integrated into the taper program?- Do you accept my insurance, and what will my estimated out-of-pocket expenses be?- What is the process if my symptoms necessitate a slower taper than initially planned?2,9
If you are unable to reach a program immediately, SAMHSA’s free, 24/7 helpline at 1-800-662-HELP provides confidential referrals to local treatment options.8
Guidance for Spouses, Parents, and Adult Children
If you are a family member reading this, you have likely witnessed the struggles of a loved one, perhaps enduring sleepless nights or questioning when to seek emergency care. Your exhaustion is valid, and your continued search for solutions is commendable.
Here are a few important considerations. First, do not encourage abrupt cessation of the medication. Stopping short-acting benzodiazepines suddenly has been linked to seizures in approximately 3% of cases, and the current standard of care from ten medical societies mandates a slow, supervised reduction, not a cold stop. If your loved one has already stopped on their own and is exhibiting tremors, confusion, or any signs of seizure activity, it is an emergency situation requiring immediate medical attention.9,10
Second, understand that your loved one is not weak. Their nervous system has adapted to a medication, often one prescribed by a doctor years ago. Approaching this as a medical condition rather than a character flaw will help maintain open communication and support.
If you cannot connect with a local program tonight, SAMHSA’s free, confidential helpline at 1-800-662-HELP is available 24/7. Make the call; your loved one does not need to be “ready” first.8
Check Your Coverage for Benzodiazepine Detox Support
Find out if your insurance covers safe, medically supervised benzodiazepine detox and treatment in Portland.
Frequently Asked Questions
Can I detox from benzodiazepines at home on my own?
Attempting benzodiazepine detox alone is highly risky. Abrupt cessation of short-acting benzodiazepines has been linked to seizures in about 3% of cases, and current clinical guidelines from ten medical societies advise against stopping these medications abruptly in dependent patients. If you are already experiencing withdrawal symptoms, please seek professional help immediately.9,10
How long does a medically supervised benzodiazepine taper take?
The duration varies based on your dose, how long you have been taking the medication, and your individual response. The 2025 joint guideline suggests starting with 5 to 10% dose reductions, generally not exceeding 25% every two weeks. For individuals on high doses for many years, a complete taper can take several months, or even longer than a year. A slower pace prioritizes safety over speed.9
I was prescribed Klonopin by my doctor. Does that mean I’m addicted?
Not necessarily. Physical dependence, where your body needs the medication to function normally, is an expected biological outcome of long-term benzodiazepine use and is clinically distinct from a substance use disorder. If you took your Klonopin as prescribed, you are dealing with a medical condition, not a moral failing. Supervised tapering is still necessary, but without judgment.9
What is BIND, and will I get it after stopping?
BIND, or Benzodiazepine-Induced Neurological Dysfunction, refers to symptoms that can persist beyond acute withdrawal. A 2023 self-reported survey of 1,207 benzodiazepine users found that over half reported symptoms like low energy, distractedness, memory issues, and anxiety lasting a year or longer. While this sample was self-selected, a slower, supervised taper is considered the primary protective factor against severe or protracted symptoms.1,9
Does insurance cover benzodiazepine detox in Portland?
Most private insurance plans (employer, marketplace, and many union plans) typically cover medically supervised detox and subsequent levels of care. However, coverage details vary regarding deductibles, in-network status, and prior authorization. The Oregon Health Plan (Medicaid) has different coverage rules, and not all private detox facilities accept it. Always contact the program directly before admission to confirm your specific coverage. SAMHSA’s free 24/7 helpline at 1-800-662-HELP can also provide assistance.8
What’s the difference between residential detox and going to a hospital?
Hospitals are designed for acute medical emergencies like seizures or severe co-occurring withdrawals, providing immediate stabilization before discharge. A benzodiazepine taper, however, is a gradual process that can take weeks to months. Residential, home-like detox offers medical supervision during the critical initial phase in a more comfortable, less clinical environment, with amenities like real beds and common areas, and integrated psychosocial support. This setting is better suited for the prolonged, gradual rhythm required for a safe benzodiazepine taper.2,9
References
- Long-term consequences of benzodiazepine-induced neurological dysfunction: A survey. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10309976/
- Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits. https://pubmed.ncbi.nlm.nih.gov/40526204/
- FDA requiring Boxed Warning updated to improve safe use of benzodiazepine drug class. https://www.fda.gov/drugs/drug-safety-and-availability/fda-requiring-boxed-warning-updated-improve-safe-use-benzodiazepine-drug-class
- Drug Overdose Deaths, Hospitalizations, Abuse & Dependency – Oregon. https://www.oregon.gov/oha/ph/diseasesconditions/injuryfatalitydata/documents/oregon-drug-overdose-report.pdf
- FDA requiring Boxed Warning updated to improve safe use of benzodiazepine drug class. https://www.fda.gov/media/142368/download
- Long-term consequences of benzodiazepine-induced neurological dysfunction: A survey. https://pmc.ncbi.nlm.nih.gov/articles/PMC10309976/
- MENTAL HEALTH CLINICAL ADVISORY GROUP LEGISLATIVE REPORT December 2022. https://www.oregon.gov/oha/HPA/DSI-Pharmacy/MHCAGDocs/Final-MHCAG-2022-Legislative-Report.pdf
- SAMHSA’s National Helpline. https://www.samhsa.gov/find-help/national-helpline
- Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits. https://pmc.ncbi.nlm.nih.gov/articles/PMC12463801/
- Benzodiazepine withdrawal syndrome seizures – PubMed. https://pubmed.ncbi.nlm.nih.gov/8773293/