Key Takeaways
- Vicodin withdrawal in Milwaukie typically starts 8 to 24 hours after the last dose, peaks between 24 and 72 hours, and resolves over 4 to 10 days.8
- Clackamas County averaged 65.5 overdose deaths and 76.2 opioid-related hospital visits annually from 2019 to 2022, making nearby residential detox a meaningful local option.9
- Compare programs on medication options like buprenorphine, methadone, naltrexone, lofexidine, and clonidine, plus whether 24-hour residential supervision is offered outside a hospital setting.1,2,7
- Look for a clear path from detox into PHP, IOP, outpatient, and alumni support, since withdrawal management alone is not enough to prevent relapse.7,8
What the First 72 Hours Off Vicodin Actually Feel Like
If you’ve stopped taking Vicodin and are experiencing withdrawal, it’s important to know that these feelings have a predictable course and will eventually end. Your body is simply reacting to the absence of hydrocodone, which it has grown accustomed to.
For short-acting opioids like Vicodin, withdrawal symptoms typically begin 8 to 24 hours after your last dose and resolve over approximately 4 to 10 days. Understanding this timeline can help manage expectations during what can feel like an endless period.8
Hours 8 to 24: Initial symptoms can be subtle, often resembling the flu. These include a runny nose, uncontrollable yawning, and a low-level anxiety that creates a feeling of tightness in the chest. You might experience alternating sweats and chills, disturbed sleep, and dilated pupils. Cravings for the drug may also begin to emerge.
Hours 24 to 72: This period marks the peak of withdrawal intensity. Symptoms can escalate to include nausea, vomiting, and diarrhea. Muscle cramps may affect your calves and lower back. The chronic pain that Vicodin once masked can return with intensity, accompanied by new symptoms specific to opioid withdrawal, such as muscle and bone pain, cold flashes with goosebumps, and uncontrollable leg movements. Insomnia is common, and anxiety can deepen into a sense of dread. Hot and cold flushes may alternate frequently.3,8
This is often the point where individuals attempting to detox alone may relapse. The body’s intense distress can be overwhelming, and Vicodin offers a known, albeit temporary, relief. Untreated withdrawal is a significant factor in returning to drug use.2
Days 4 to 10: The severity of symptoms generally decreases during this phase. Sleep may gradually improve, and muscle cramps can subside. You might feel exhausted and emotionally vulnerable, which is a normal part of the recovery process. Support from others who understand can be crucial during this time.
It’s important to remember that these are predictable physiological responses. Medical supervision and medication can significantly alleviate these symptoms, making the process more manageable.
Why Milwaukie and Clackamas County Need a Closer Door
For residents of Milwaukie seeking help for Vicodin dependence, accessible local support is vital. The statistics within Clackamas County highlight the urgent need for nearby treatment options.
Between 2019 and 2022, Clackamas County experienced an average of 65.5 overdose deaths annually, equating to approximately 15.5 deaths per 100,000 people. During the same period, the county recorded an average of 76.2 opioid-related hospital visits per year, or 18.1 per 100,000 residents. These figures represent individuals within the community, underscoring the widespread impact of opioid use.9
This data suggests a critical gap between an individual’s decision to stop using Vicodin and their ability to access medical care. While emergency rooms can stabilize an overdose, they are not equipped for comprehensive detox. An ER visit addresses the immediate crisis but often sends individuals home without a structured plan, leaving them vulnerable to relapse as cravings return.
A residential detox facility located close to home can significantly alter this dynamic. It eliminates the difficult choice between seeking medical care and being near family. Family visits become feasible, and the journey home after discharge is less daunting. Furthermore, local clinical teams are familiar with local outpatient programs, pharmacies, and recovery meetings, ensuring a seamless transition to ongoing care.
What Medical Detox Means When You’re Not in a Hospital Bed
Many people associate medical detox with a hospital environment, complete with fluorescent lights and the constant beeping of machines. This image can deter individuals from seeking help, as they may not feel “sick enough” for a hospital, and often, they are right.
There is a specialized level of care designed for this situation: medically monitored residential detox. This involves 24-hour medical supervision in a comfortable, home-like setting, with nurses on staff and a physician overseeing treatment. Medications are readily available to manage symptoms as they arise. This approach offers the same medical oversight without the typical hospital atmosphere.7
Practically, this means a private bedroom instead of a gurney, access to a kitchen with nourishing food, and common areas where individuals undergoing similar experiences can connect. Vital signs are regularly monitored, and a withdrawal scale, such as the SOWS, is used to assess symptoms every few hours, guiding medication adjustments.8
Clinically, this is referred to as sub-acute care. In simpler terms, it’s medical care outside of a hospital setting. It’s particularly suitable for opioid withdrawal because, while hydrocodone withdrawal can be severe, it is rarely life-threatening on its own. However, it is often unmanageable without support. A residential team can monitor and treat symptoms like a rapid pulse, high blood pressure, diarrhea, vomiting, and intense anxiety in real-time.7
Crucially, you won’t have to navigate pharmacies at odd hours for necessary medication. It’s already on-site, prescribed, and integrated into your personalized treatment plan from the moment you arrive. You can sleep in a comfortable bed, eat when you’re able, and receive overnight check-ins. When the most challenging moments occur, support is immediately available.
This form of medical detox provides the same safety net as a hospital but in a more conducive and less intimidating environment.
The Medications That Do the Heavy Lifting
Buprenorphine, Methadone, and Naltrexone: Three Tools, Three Jobs
You don’t have to endure withdrawal without help. The FDA has approved three medications for opioid use disorder, each serving a distinct purpose at different stages of recovery from Vicodin dependence. A skilled detox team will select the most appropriate medication based on your individual needs.1
Buprenorphine: This medication is frequently used early in the detox process for individuals withdrawing from Vicodin. It partially binds to the same receptors as hydrocodone, effectively reducing cravings and alleviating withdrawal symptoms without producing a euphoric high. This can lead to decreased muscle aches, reduced anxiety, and improved sleep. Buprenorphine is typically initiated after a sufficient period has passed since the last Vicodin dose to avoid precipitating worse withdrawal. Once stable, the dosage can be gradually reduced over several days or maintained for a longer period if clinically indicated for ongoing recovery.
Methadone: Methadone is a long-acting opioid that replaces Vicodin and is then slowly tapered. It provides a smoother, more controlled reduction in opioid dependence, preventing the abrupt onset of severe withdrawal symptoms. In Oregon, methadone is strictly regulated and dispensed through specialized programs, making it a targeted treatment option for specific cases.5
Naltrexone: Naltrexone is used after withdrawal is complete and the body is free of opioids. It works by blocking opioid receptors entirely, meaning that if Vicodin were used again, the euphoric effects would not be felt. This medication helps protect the progress made in recovery. An extended-release injectable form is available, providing about a month of coverage and reducing the need for daily medication decisions.
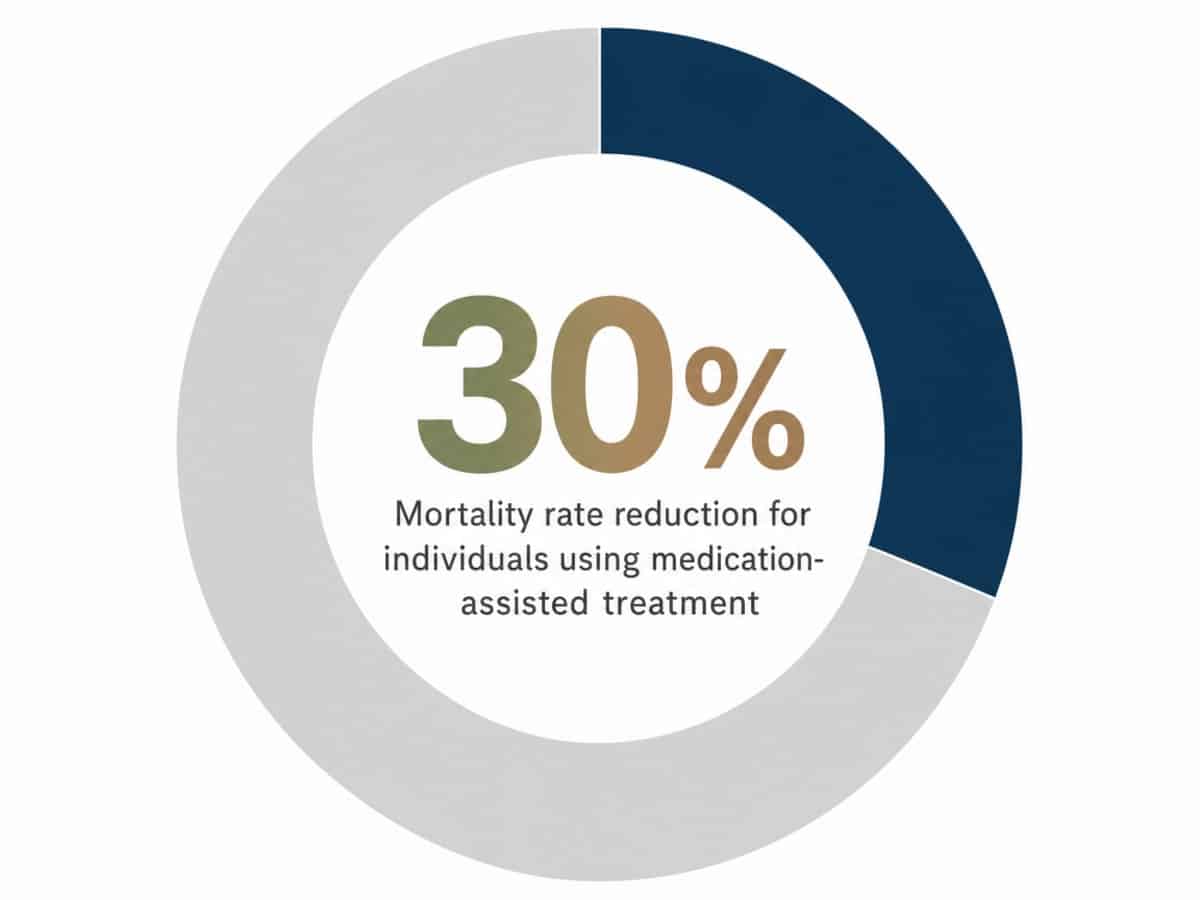
These medications are crucial not just for comfort, but for improving outcomes. The Oregon Health Authority notes that individuals receiving medication-assisted treatment have up to a 30% reduced mortality rate compared to those attempting recovery without it. This statistic highlights the life-saving potential of these medical interventions.10
Lofexidine, Clonidine, and Calming a Nervous System in Overdrive
Not all medications used in Vicodin detox are opioids. Some of the most effective treatments target the nervous system, which goes into overdrive when hydrocodone is no longer present.
This physiological response is clinically known as noradrenergic hyperactivity. Essentially, your body has relied on Vicodin to suppress certain functions, and when the drug is removed, these functions rebound. Symptoms include a racing heart, elevated blood pressure, sweating, restless legs, and intense physical anxiety. This is where medications like lofexidine and clonidine become beneficial.
Both are alpha-2 agonists and have demonstrated effectiveness in reducing the severity of symptoms during short-acting opioid withdrawal, outperforming placebo in clinical trials. Lofexidine is a newer medication specifically approved for opioid withdrawal, while clonidine has been used off-label for decades and remains a common treatment in detox settings.2,8
These medications help to slow a racing heart, reduce excessive sweating, ease cramping, and improve sleep. Unlike buprenorphine or methadone, they do not replace the opioid but rather mitigate the nervous system’s extreme reaction. They are often used in conjunction with other medications or as a primary treatment when opioid replacement therapy is not suitable.
Additionally, supportive medications may be prescribed for specific symptoms such as nausea, diarrhea, or persistent insomnia. These are not intended to create a high or substitute one drug for another, but rather to provide comfort and stability, allowing the nervous system to recover without being overwhelmed.
Who Walks Through the Door: Four People, One Withdrawal
Vicodin dependence affects a diverse range of individuals. While the chemical process of withdrawal remains consistent, the personal journey leading to treatment shapes the specific support needed from a care team.
The post-surgery patient who never stopped: You might have started Vicodin for legitimate pain after a surgery or injury. When the prescription ended, the pain returned, and you found other ways to obtain the medication. You may not identify as having an addiction, but rather as someone who never fully recovered. It’s important to understand that physical dependence on hydrocodone is a recognized outcome of legitimate prescribing, not a personal failing. The same medications used for any opioid use disorder can effectively help you.3
The working professional hiding it: You maintain a demanding career, and no one suspects your struggle with Vicodin, which you’ve managed to conceal for years. The shame can sometimes feel more intense than the withdrawal itself. For you, a residential setting that doesn’t resemble a hospital is crucial, as is a discreet team experienced in supporting individuals in similar situations.
The person who switched: Perhaps Vicodin wasn’t your first opioid. You might have previously used heroin, oxycodone, or fentanyl, and are now using Vicodin to maintain stability. While the detox plan will be similar, the treatment team will adjust medication dosages and strategies to account for your body’s specific tolerance and history.
The family member making the call: You are not experiencing withdrawal, but you are deeply concerned for a loved one. You’ve likely spent sleepless nights researching options. The most impactful action you can take is to continue gathering information and make that initial phone call. Your loved one could be admitted for care as early as tomorrow, without having to initiate the call themselves.
Why Detox Alone Is the Single Biggest Reason People Return to Vicodin
A crucial aspect often overlooked is that completing withdrawal is not the same as achieving full recovery. Detoxification removes the drug from your system, but it does not address the underlying patterns or triggers that led to drug use in the first place.
Clinical guidelines explicitly state that detoxification alone is insufficient treatment, and individuals who complete withdrawal management without a subsequent treatment plan frequently relapse. This is not a moral failing but a consequence of neurochemistry and circumstance. Your brain has learned over time that hydrocodone provides relief from pain, stress, or discomfort. Five days of medication cannot erase these learned associations; it merely provides a clean slate.7,8
Without a plan, the days following discharge can be challenging. While acute symptoms subside, a lingering sense of unease, poor sleep, low mood, and restlessness can persist. Cravings may return in waves, feeling less like a desire and more like a strong memory. The first difficult conversation, a minor physical ache, or a lonely evening can trigger the brain to recall the “solution” of Vicodin. This is often when most relapses occur.2
The solution isn’t simply willpower. It involves ensuring that the next step in treatment begins before the current one ends. This could mean connecting with a counselor, continuing a medication plan beyond the initial detox period, or joining a support group. When detox transitions seamlessly into ongoing care, rather than ending abruptly at your front door, the chances of sustained recovery significantly improve. A program that integrates aftercare is not an optional add-on; it is an essential component of effective treatment.
The Staircase After Detox: PHP, IOP, Outpatient, Alumni
Think of recovery as a staircase rather than a finish line. Detox is the initial step. Each subsequent step requires less time commitment but offers your nervous system more opportunities to adapt to life without Vicodin. Clinical guidelines emphasize that withdrawal management alone is insufficient; it must lead to ongoing treatment for lasting recovery.7
Partial Hospitalization Program (PHP): For many, this is the immediate step after detox. You spend a significant portion of your day in structured treatment, including group therapy, individual counseling, and medication management. Psychiatric care for co-occurring anxiety or depression, often masked by hydrocodone use, may also be included. You return home or to supportive housing for the evenings. This provides a gentle transition, maintaining medical oversight and a consistent medication plan.
Intensive Outpatient Program (IOP): This involves several hours of treatment a few days a week. You begin to reintegrate into daily life, returning to work, family responsibilities, and household tasks. The structure remains, with regular group sessions and individual counseling, allowing you to identify and address real-life triggers as they emerge.
Standard Outpatient: This level of care typically involves weekly or bi-weekly sessions with a counselor. If you are on buprenorphine or naltrexone, you will continue to see a prescriber to manage your medication as long as it remains beneficial for your recovery.1
Alumni: This refers to a community of individuals who have completed treatment and continue to support each other. It’s not a formal program but a valuable network that provides ongoing connection and support, especially during challenging times.
The goal is not to complete every single step, but to ensure you are always engaged in some form of supportive care, avoiding periods without any structured support.
What to Bring, What to Expect, and How to Call
The initial phone call for intake is often quicker than anticipated, typically lasting about fifteen minutes. During this call, you’ll be asked about your substance use, including the type, amount, duration, and last dose of Vicodin. Questions about other medications, existing diagnoses, and your current safety will also be covered. The purpose of these questions is not to judge, but to ensure that the treatment plan and available resources are appropriate for your needs.
What to bring: You’ll need a photo ID and your insurance card, if applicable. Most insurance plans cover residential detox, though it’s important to inquire about specific coverage details, as the Oregon Health Plan can sometimes be an exception. A list of any current medications, including dosages, is also necessary. Pack comfortable clothing for about a week, such as sweatpants, t-shirts, a hoodie, and slippers. Personal hygiene items like a toothbrush, glasses, contacts and solution, and prescription medications in their original bottles should be included. A book or journal can be helpful. It’s best to leave laptops, work phones, and any other distracting electronic devices at home, as the focus of the week is on disconnection and healing.
What to expect on day one: Upon arrival, a nurse will check your vital signs and conduct a more detailed review of your medical history. A physician will then finalize your treatment plan and issue initial medication orders. You’ll be introduced to the staff on duty and shown to your room. If you are already experiencing withdrawal symptoms upon arrival, the first dose of medication to alleviate discomfort is usually administered within the hour.8
How to call: If you are in the Milwaukie area and ready to speak with someone, Pacific Crest Trail Detox accepts intake calls directly. Alternatively, if you prefer a national resource that can connect you to local options, the SAMHSA National Helpline offers free, confidential assistance 24 hours a day, every day of the year.6
You don’t need to be entirely certain about seeking help; simply making the call is a significant first step.
Check Your Coverage for Safe Vicodin Detox
See if your insurance covers a safe, supportive Vicodin detox in Milwaukie today.
Frequently Asked Questions
How long does Vicodin withdrawal last?
For short-acting opioids like Vicodin, withdrawal symptoms typically begin 8 to 24 hours after the last dose and generally resolve within 4 to 10 days. The most intense period is usually during days two and three, characterized by peak nausea, cramps, and deep aches. While the severity decreases afterward, it can take another week or two for sleep patterns and energy levels to return to normal.8
Is it safe to detox from Vicodin at home?
While hydrocodone withdrawal is rarely life-threatening on its own, managing it alone can be extremely difficult. Untreated symptoms are a primary reason individuals return to drug use. Detoxing at home lacks access to medications that can alleviate cravings or calm an overactive nervous system. A medically supervised setting provides these essential tools immediately and offers continuous monitoring throughout the night.2
What medications are used during a Vicodin detox?
Three FDA-approved medications are used to treat opioid use disorder: buprenorphine, methadone, and naltrexone, each applied at different stages of recovery. Additionally, alpha-2 agonists like lofexidine and clonidine are used to manage nervous system symptoms such as a racing heart, sweating, and restless legs, having shown superior efficacy to placebo in trials for short-acting opioid withdrawal. Supportive medications for nausea, diarrhea, and insomnia are also part of a comprehensive treatment plan.1,2
Do I have to go to a hospital for medical detox?
No. Clinical guidelines outline medically monitored residential detox, which provides 24-hour medical supervision in a comfortable, home-like environment, with nurses on staff and a physician overseeing medication management. This approach offers the same level of medical oversight without the typical hospital setting, making it an ideal fit for most individuals withdrawing from Vicodin, as it provides a strong safety net without the clinical atmosphere.7
What happens after detox ends?
Detoxification removes the drug from your system but is not a complete treatment on its own. Most individuals transition through various levels of care, such as partial hospitalization, intensive outpatient, and standard outpatient programs, with ongoing medication and counseling. Alumni groups provide continued support thereafter. The goal is to maintain continuous engagement in some form of care, as having a plan for the days following discharge is critical for sustained recovery.7
Will my insurance cover detox in Milwaukie?
Most commercial insurance plans typically cover residential medical detox, though the specifics of coverage can vary by policy. The Oregon Health Plan is a common exception, so it’s advisable to inquire about this upfront. The quickest way to determine your coverage is through a brief intake call, where your benefits can be verified. Alternatively, the SAMHSA National Helpline is a free, 24-hour national resource that can help you find local options.6
References
- Information about Medications for Opioid Use Disorder (MOUD). https://www.fda.gov/drugs/information-drug-class/information-about-medication-assisted-treatment-mat
- Review article: Effective management of opioid withdrawal symptoms. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6590307/
- Prescription Opioids DrugFacts | National Institute on Drug Abuse. https://nida.nih.gov/publications/drugfacts/prescription-opioids
- Opioid Medications – FDA. https://www.fda.gov/drugs/information-drug-class/opioid-medications
- Medication-Assisted Treatment for Opioid Use Disorder. https://www.oregon.gov/oha/HSD/AMH/Pages/MAT.aspx
- SAMHSA’s National Helpline. https://www.samhsa.gov/find-help/national-helpline
- Quick Guide For Clinicians Based on TIP 45—Detoxification and Substance Abuse Treatment. https://nida.nih.gov/sites/default/files/samhsa_detoxification_and_substance_abuse_treatment.pdf
- Clinical Guidelines for Withdrawal Management and Treatment of Drug Dependence in Closed Settings. https://www.ncbi.nlm.nih.gov/books/NBK310652/
- County-level data for ADPC Committees – Oregon.gov. https://www.oregon.gov/adpc/SiteAssets/Lists/MeetingEvents/EditForm/ADPC%20County%20Overdose%20Data%204.9.24.pdf
- Oregon Health Authority : Medication-Assisted Treatment for Opioid Addiction. https://www.oregon.gov/oha/hsd/amh/pages/mat.aspx