
Key Takeaways
- Outpatient programs in Milwaukie are part of Clackamas County’s OHA-certified network, with publicly listed providers covering standard outpatient, IOP, co-occurring care, and DUII treatment.1
- Oregon evidence shows outpatient care paired with medication for opioid use disorder can perform favorably against more intensive settings, making it a clinically sound choice rather than a lighter one.3
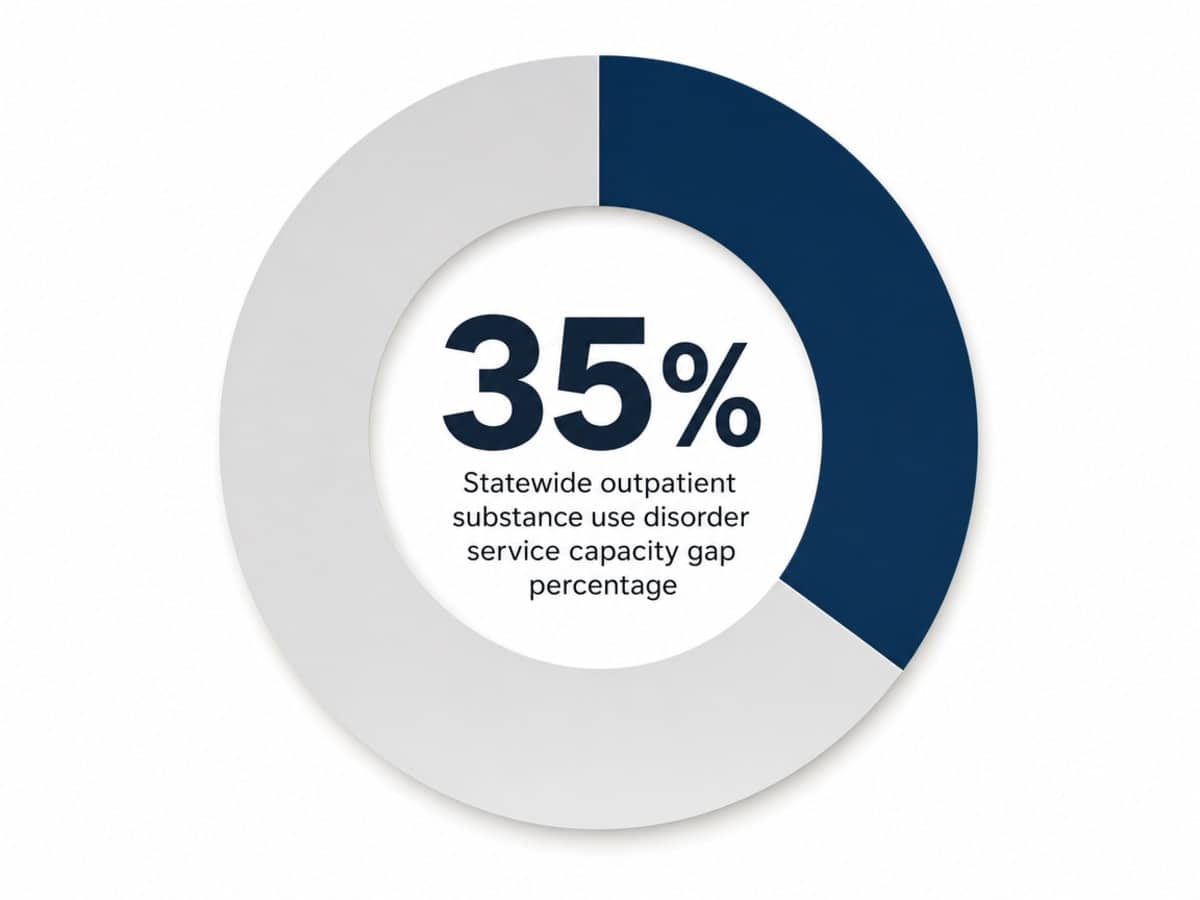
- Capacity is tight statewide, with a 35% gap between need and available outpatient units, so calling several certified providers quickly protects the window between deciding and starting.4
- Before committing, compare certifications, ASAM-based level-of-care decisions, on-site medication options, co-occurring screening, weekly schedule structure, and step-down planning across Milwaukie programs.6,8
When outpatient is the right-sized choice, not the lighter one
You’re holding a hard question in one hand and a full life in the other. A job that needs you on Monday. Kids who expect dinner. A reputation you’ve spent years building. And somewhere underneath all of that, a quieter truth — drinking or using has stopped working, and you know it.
Here’s what often gets lost in the noise: outpatient treatment isn’t the watered-down version of recovery. For many people in Milwaukie and the wider Portland metro area, it’s the right-sized version. You sleep at home. You stay close to your people. You keep showing up to the things that matter while a clinical team helps you change the one thing that doesn’t.
That framing matters because the choice in front of you isn’t “serious treatment versus easy treatment.” It’s matching the level of care to what you actually need. Oregon classifies outpatient programs along the same clinical levels used nationally, and the state’s certified providers follow those standards through the Oregon Health Authority. A structured outpatient program — sometimes called an intensive outpatient program, or IOP — can deliver real therapy, medication support when it’s appropriate, and accountability, without asking you to disappear from your life for a month.8
If you’re a working professional, a parent, a veteran, or someone who simply values their privacy, that combination is not a compromise. It’s a plan. The rest of this guide walks you through what outpatient looks like in Milwaukie, how to read the local landscape, and the questions that separate certified care from a polished website.
What outpatient care actually looks like in Milwaukie
The local landscape: OHA-certified providers in Clackamas County
Milwaukie sits inside Clackamas County, which means the outpatient programs you’ll find here are part of a regulated network — not a free-for-all of unverified clinics. The Oregon Health Authority publishes a directory of certified substance use disorder providers, and Milwaukie shows up in it. You can see specific addresses, like the cluster of services near 6902 SE Lake Road, with checkboxes indicating which levels of care each site is licensed to deliver: outpatient SUD services, intensive outpatient services, co-occurring disorder care, and DUII treatment among them.1
That directory is more useful than it looks. When a provider’s listing shows certification for both standard outpatient and IOP, it tells you the program can step you up or down without sending you somewhere new. When it shows DUII certification, it tells you the program is set up to handle court reporting requirements. When it shows co-occurring disorders, it tells you they’re staffed to treat depression, anxiety, or trauma alongside substance use.
Oregon’s outpatient framework also covers more than just drugs and alcohol — the state’s behavioral health outpatient programs include mental health and problem gambling services within the same regulatory category. For you, that translates into a practical reality: a certified Milwaukie program is more likely to treat the whole picture than a generic recovery storefront would.8
A typical IOP week: hours, format, and the rhythm you can plan around
Let’s get concrete, because “intensive outpatient” sounds vague until you put it on a calendar. An IOP delivers a set number of structured hours each week — usually around nine — split across individual therapy, group sessions, and family therapy. Many Milwaukie-area programs schedule those hours across three evenings, which is how working adults actually fit treatment into a life that already has meetings, school pickups, and a commute.5
Picture a Tuesday, Wednesday, and Thursday from 6:00 to 9:00 p.m. One block is group — eight or so people working through the same kinds of triggers and the same kinds of weeks. Another block is skills-focused: how to handle a craving on a Friday night, how to talk to your partner about what changed, how to sit with a feeling instead of drinking it away. SAMHSA describes this as a mix of one-on-one appointments, group sessions, and learning coping skills, often with telehealth options layered in for flexibility.7
You’ll also have an individual therapy hour each week, usually scheduled around your work day. Family sessions show up every other week or once a month, depending on the program and what you and your people are ready for.
Here’s the part that gets missed: the hours are structured, but the rest of your week is yours. You sleep in your bed. You eat breakfast with your kids. You go to work on Monday. The treatment runs alongside your life instead of replacing it — and for a lot of people, that’s exactly why it sticks. You’re practicing recovery in the environment you actually live in, not a controlled bubble you’ll eventually have to leave.
How outpatient differs from detox, residential, and partial hospitalization
Treatment isn’t a single thing — it’s a ladder. Knowing where outpatient sits on that ladder helps you figure out where you actually need to start.
Medical detox is the bottom rung when withdrawal is the immediate risk. If you’re drinking heavily every day or using benzodiazepines like Xanax or Klonopin, stopping cold can be dangerous, and a medically supervised detox handles that first stretch safely. It’s short — usually days, not weeks — and it’s not therapy. It’s stabilization.
Residential treatment is the most immersive: you live on-site for two to four weeks or longer, and treatment fills the day. It’s the right call when home isn’t safe, when triggers are everywhere, or when earlier outpatient attempts haven’t held.
Partial hospitalization, or PHP, sits between residential and IOP. You’re at the program five or six hours a day, five days a week, but you sleep at home. Think of it as a step-down from residential or a step-up from IOP when more support is needed.
Standard outpatient is lighter still — usually one to two hours a week of therapy, often after you’ve completed an IOP. Oregon classifies these levels using ASAM criteria, the same framework used nationally for matching the intensity of care to the severity of need. The right rung isn’t the highest one. It’s the one that meets you where you are.6
The Oregon evidence: why outpatient with medication holds its own
If you’ve ever heard someone say outpatient is for people who “aren’t serious yet,” here’s a finding worth sitting with. A 2022 peer-reviewed study followed Oregon adults with opioid use disorder across different treatment settings and found that outpatient care, when paired with medication for opioid use disorder, performed favorably compared to other settings — including residential. That’s a meaningful directional signal in your own state, in your own system.3
A few caveats matter, because honest evidence beats reassuring evidence. The study looked at Oregon patients with opioid use disorder specifically — not alcohol, not stimulants, not every substance someone might be working through. It was observational, meaning researchers tracked what happened in real care rather than randomly assigning people to treatment. People who choose outpatient and people who enter residential aren’t always the same on day one, and good researchers acknowledge that. What the data shows is a pattern: outpatient plus the right medication can hold its own — and sometimes outperform — more intensive settings for the population studied.
What does this mean for you, sitting in Milwaukie weighing your options? It means choosing outpatient isn’t choosing less care. It’s choosing a setting where, for many people, the evidence supports the path — especially when medication is part of the plan and the program is built to deliver both. Ask about medication early. Ask whether the program prescribes on-site or coordinates with a partner provider. Ask how they decide who’s a candidate. Those are the questions that turn a directional study into a practical decision.
Why timing matters: capacity, waitlists, and getting in the door
Here’s something that doesn’t get said often enough: the moment you decide you’re ready is the moment to call. Not next month, when the calendar clears. Not after the holidays. Now — because Oregon’s outpatient system, as good as it is in pockets, is stretched.
A 2023 OHSU gap analysis put real numbers on what providers already feel. Across Oregon, the state needs roughly 586 outpatient SUD service capacity units to meet demand. It has 383. That leaves a gap of 203 — about 35% of what’s needed simply isn’t there yet. Clackamas County is part of that picture, which means a Milwaukie program with an open intake slot today might have a two- or three-week wait by the end of the month.4
What that means for you, practically:
- Call more than one program. If the first certified provider has a wait, the second might not. Use the OHA directory as your starting list, not a single phone number.
- Ask for the soonest intake assessment, even if treatment starts later. Many programs can get you in for an initial evaluation within days, then schedule your group start when a cohort opens.
- Ask about telehealth bridges. Some programs offer individual sessions or check-ins remotely while you wait for an in-person group seat.
- If you’re stepping down from detox or a hospital, push for a warm handoff. Direct provider-to-provider referrals often move faster than calling cold.
The window between deciding and starting is fragile. Protect it. Make the calls today, and let the system catch up to your readiness instead of the other way around.
Medication support in outpatient settings: what’s available and where
Medication is one of the biggest reasons outpatient care has come into its own. The right prescription, paired with therapy, can quiet the cravings enough that you can actually do the work — show up to group, sit with hard feelings, and rebuild a life that doesn’t revolve around the next drink or pill.
For opioid use disorder, two medications come up most often. Buprenorphine, often dispensed as Suboxone, can be prescribed by a wide range of certified providers and is the more flexible option for outpatient settings. Methadone is more tightly regulated — Oregon allows it only through approved opioid treatment programs, not at every outpatient clinic. That distinction matters when you’re picking a program. If methadone is the right fit for you, you’ll need a provider with that specific license, or a clinic that coordinates closely with one. If buprenorphine is on the table, your range of certified Milwaukie options widens considerably.11
For alcohol use disorder, medications like naltrexone and acamprosate can reduce cravings and the reward of drinking. They’re often underused, even though they’re well-studied. Ask directly: Do you prescribe medication for alcohol use disorder, or coordinate with a provider who does? A program that says yes is one that’s keeping the full toolbox available — not just the ones that are easiest to schedule.
Screening for what else is going on: co-occurring conditions and polysubstance use
Substance use rarely travels alone. The drinking that started after a divorce. The pills that quieted a panic that was already there. The stimulant use that’s been propping up a depression no one named. If any of that sounds familiar, you’re not unusual — you’re the rule, not the exception.
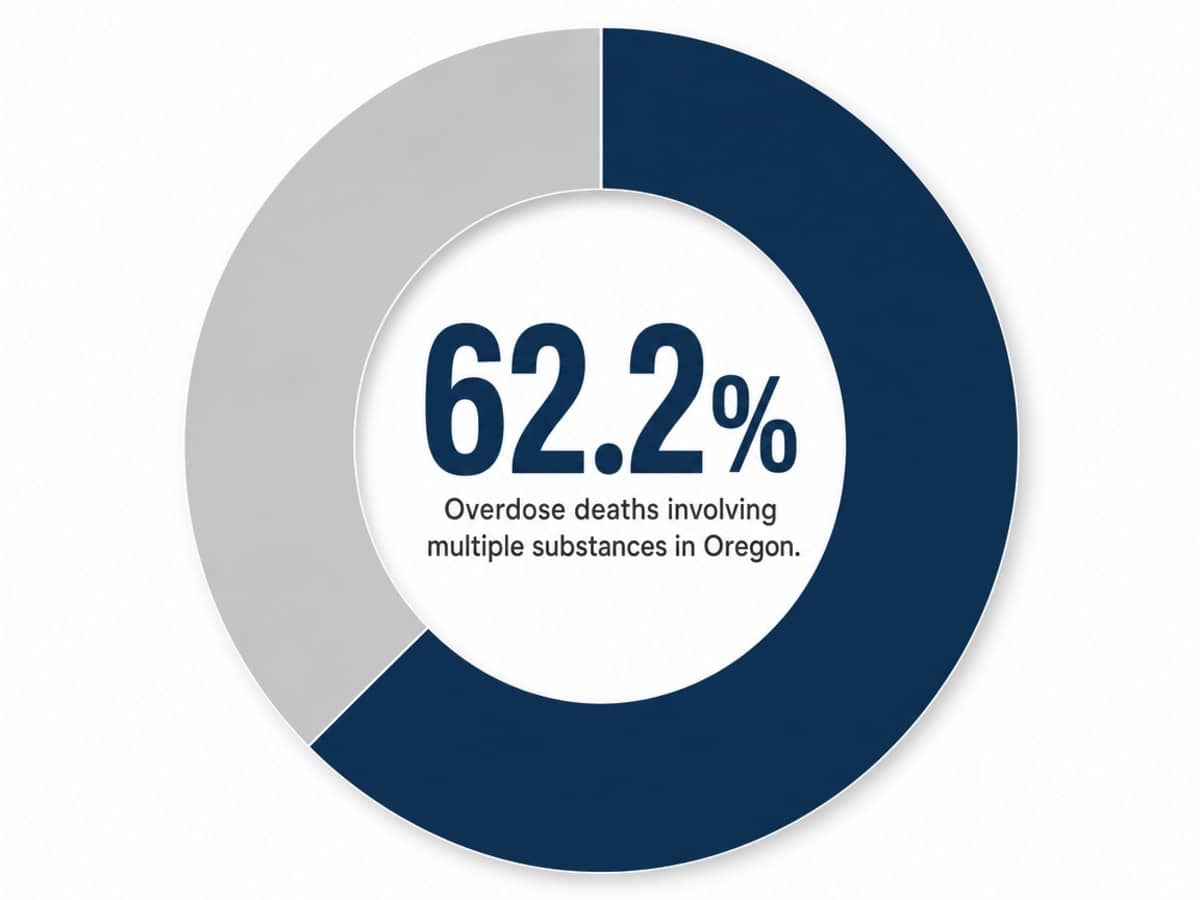
That’s why a strong outpatient program in Milwaukie spends real time at intake asking about what else is going on anxiety, depression, PTSD, ADHD and old trauma you’ve never said out loud. And it asks about every substance, not just the one that brought you in. Oregon’s most recent integration data shows that polysubstance use was a factor in 62.2% of overdose deaths statewide — more than half of fatal cases involved more than one drug, often combinations the person didn’t fully realize they were mixing. That isn’t shared here to scare you. It’s shared because it changes how a good program screens you.2
Ask directly: How do you assess for mental health conditions alongside substance use? Do you treat both, or refer out? Oregon’s certified outpatient framework explicitly includes co-occurring care within the same regulatory category. A program that handles both under one roof — therapists, prescribers, and groups that understand the overlap — saves you the exhausting work of telling your story twice to two different teams.8
How to vet a Milwaukie outpatient program
Six questions that separate certified care from marketing language
Every treatment website looks reassuring. Soft photography, language about “personalized care,” maybe a tree on a hillside. That’s not how you tell a strong program from a weak one. These six questions will.
- Are you certified by the Oregon Health Authority, and for which specific levels of care? The OHA directory tells you whether a provider is certified for outpatient SUD services, intensive outpatient, co-occurring disorders, and DUII — and you can check it yourself before the call. If a program can’t name its certifications clearly, that’s your answer.1
- How do you decide which level of care fits me? A credible program uses ASAM criteria — the standardized framework Oregon uses to match treatment intensity to the severity of need. Listen for words like “assessment,” “dimensions,” or “ASAM level.” Vague answers about “what feels right” are a flag.6
- Do you prescribe medication on-site, or coordinate with a provider who does? For opioids, that means buprenorphine access — and methadone coordination if it’s clinically indicated, since Oregon allows methadone only through approved opioid treatment programs. For alcohol, ask specifically about naltrexone or acamprosate.11
- How do you screen for mental health and other substances at intake? A program that treats co-occurring conditions under one roof saves you from telling your story to two unconnected teams.8
- What does a typical week look like — hours, format, and group size? Expect roughly nine structured hours weekly across individual, group, and family therapy.5
- What happens after I finish? Strong programs name their step-down plan, alumni groups, or continuing care — not a discharge date and a handshake.
Privacy, work, and family logistics: what to ask intake
The clinical questions matter. So do the practical ones — the ones that decide whether you can actually keep showing up. Bring these to your intake call, and don’t apologize for asking.
On privacy. Ask how the program protects your records and who, exactly, has access. Federal rules around substance use treatment records are stricter than standard medical privacy, and a good intake coordinator will explain that without flinching. Ask whether anything appears on a background check (it doesn’t, when you’re a voluntary patient). Ask what shows up on insurance statements that go to your home — and whether you can switch to electronic-only delivery.
On work. If you need an accommodation, ask whether the program writes letters for FMLA, employee assistance programs, or short-term leave — without disclosing diagnosis specifics to your employer. Ask if evening groups are running consistently, not just “sometimes.” Ask whether telehealth is available for weeks you travel.
On family. Ask when family sessions start and how often they run. Ask whether your partner or adult kids can join a separate family education group, which many programs offer alongside individual family therapy. Ask what to tell young children — most clinicians will help you script that conversation.
On the basics. Parking, transit access from the Orange Line, what to bring the first night, whether childcare during groups is something they coordinate. None of these are small. They’re the difference between a plan that works on paper and a plan that survives Tuesday.
Stepping down from detox or stepping up from outpatient: care as a continuum
Recovery isn’t one program. It’s a sequence of right-sized supports, and the strongest outcomes usually come from people who move between levels as their needs change — not from people who pick one box and stay in it.
If you’re coming out of medical detox, the days right after are when the work actually begins. Detox handles the body. It doesn’t handle the Tuesday afternoon when the urge hits at your desk. A direct handoff into an IOP — ideally arranged before you discharge — keeps that fragile window from becoming a relapse. Ask your detox team to coordinate the intake call while you’re still on-site. Warm referrals beat phone trees.
If you’ve been in standard outpatient and the wheels are wobbling — missed sessions, a slip, a partner who’s worried — that’s not failure. That’s information. Stepping up to an IOP, or even a partial hospitalization program, is how the system is supposed to work. Oregon’s ASAM-aligned framework is built to let you move between levels of care based on what’s actually happening in your life.6
The point isn’t to climb a ladder once and be done. It’s to stay close to the support that fits this season — and to let care follow you from detox into your everyday life, through every season after.
Taking the next step
You’ve read enough. The next move is small and specific: pick up the phone and ask for an intake assessment.
Start with the Oregon Health Authority directory of certified providers in Milwaukie, and call two or three programs in the same afternoon. Ask each one when their next assessment slot opens. Ask about evening IOP groups, medication options, and how they handle co-occurring anxiety, depression, or trauma alongside substance use. Take notes on who answers the practical questions clearly and who gets vague.1
If you’re already in detox or stepping out of a hospital stay, ask your current team to coordinate the handoff before you discharge. Warm referrals move faster than cold ones, and that first week after detox is when the structure of an outpatient program does its most important work.
You don’t have to disappear from your life to get well. You can keep your job, stay in your home, show up for your kids, and still do the real work of recovery — with a team that understands the Milwaukie landscape. Pacific Crest Trail Detox is one place to start that conversation.
Check Your Coverage for Outpatient Drug Support
See if your insurance covers discreet outpatient treatment in Milwaukie.
Frequently Asked Questions
Will my insurance cover an outpatient drug program in Milwaukie?
Most commercial insurance plans cover outpatient substance use treatment, including IOP, when you go through an Oregon Health Authority certified provider. Call the program’s intake line and ask them to verify your benefits before your first session — they’ll check copays, session limits, and any pre-authorization. Ask whether statements mailed home can switch to electronic delivery for added privacy.1
How do I keep outpatient treatment private from my employer?
Federal rules around substance use records are stricter than standard medical privacy, and a voluntary outpatient program does not appear on a background check. Your employer learns nothing unless you choose to share. If you need time-off paperwork, ask the program to write FMLA or employee assistance letters that confirm care without naming your diagnosis. Evening IOP groups also let many people attend without missing work at all.
Can I attend an outpatient program if I have a DUII requirement?
Yes. The OHA directory marks which Milwaukie providers are certified specifically for DUII treatment, meaning they handle the assessments, hours, and court reporting your case requires. When you call, say upfront that you have a DUII obligation and ask whether they file directly with the court or treatment court program. That detail saves weeks of back-and-forth and keeps you in compliance while you do the actual recovery work.1
Is telehealth an option for outpatient drug treatment in the Portland metro area?
Often, yes. SAMHSA recognizes telehealth as a standard delivery option for outpatient and IOP services, including individual sessions and some group meetings. Many Milwaukie-area programs blend in-person evening groups with remote individual therapy or check-ins for travel weeks. Ask the program directly which sessions can be virtual, whether your state of residence affects eligibility, and how they handle medication appointments when you’re out of town.7
Can my spouse, partner, or family be involved in my outpatient care?
Family involvement is a core part of strong IOPs — structured family therapy is one of the three pillars alongside individual and group sessions. Expect family sessions every other week or monthly, with separate education groups for partners and adult children at many programs. You stay in control of what’s shared. Ask intake when family work begins, who’s invited, and whether sessions are offered in-person, by video, or both.5
Do I need medical detox before starting an outpatient program?
It depends on what you’re using and how much. Heavy daily alcohol use and benzodiazepines like Xanax or Klonopin can make unsupervised withdrawal dangerous — medical detox comes first, then outpatient. For opioids, many people start outpatient directly with buprenorphine, while methadone requires an approved opioid treatment program. The honest answer: a clinical assessment decides. Call a certified provider and let them evaluate before you stop on your own.11
References
- [PDF] Oregon Substance Use Disorders Services Directory. https://www.oregon.gov/oha/HSD/AMH/docs/provider-directory.pdf
- [PDF] Substance Use Disorder Integration Report – Oregon.gov. https://www.oregon.gov/oha/HSD/AMH/DataReports/SUD-Integration-Report.pdf
- Association between treatment setting and outcomes among oregon opioid use disorder patients. https://pmc.ncbi.nlm.nih.gov/articles/PMC9389731/
- [PDF] Oregon Substance Use Disorder (SUD) Services Inventory & Gap Analysis. https://www.oregon.gov/adpc/SiteAssets/Lists/MeetingEvents/EditForm/OHSU%20Gap%20Analysis%20Oregon%20ADPC.pdf
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Medicaid Policy – ASAM Implementation of the SUD 1115 Waiver. https://www.oregon.gov/oha/hsd/medicaid-policy/pages/asam.aspx
- Treatment Types for Mental Health, Drugs and Alcohol | SAMHSA. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Behavioral Health Outpatient Treatment Programs … – Oregon.gov. https://www.oregon.gov/oha/hsd/amh-lc/pages/op.aspx
- Milwaukie city, Oregon – U.S. Census Bureau QuickFacts. https://www.census.gov/quickfacts/fact/table/milwaukiecityoregon/RHI225224
- Oregon Substance Use Disorder Services Inventory and Gap Analysis. https://www.oregon.gov/oha/HSD/AMH/DataReports/SUD-Gap-Analysis-Inventory-Report.pdf
- Oregon Health Authority : Medication-Assisted Treatment for Opioid …. https://www.oregon.gov/oha/hsd/amh/pages/mat.aspx


