
Key Takeaways
- Intensive outpatient programs in the Portland metro deliver evening groups, individual counseling, and medication options that match inpatient outcomes for most people 1.
- Oregon’s care continuum runs from medical detox through PHP, IOP, and standard outpatient, so the right starting rung depends on physical dependence and home stability.
- Federal 42 CFR Part 2 protections, evening cohorts, and telehealth let working professionals protect privacy, licenses, and PTO while still completing real clinical work.
- Before enrolling, compare OHA certification, MAT integration, outcome tracking, wait times, and insurance or OHP acceptance using the state’s provider directory 9.
Treatment that fits a working life in Portland
You have a job that matters to you. A calendar that doesn’t bend. Maybe a license to protect, a team that depends on you, or a family who still thinks the late nights are just deadlines. And somewhere underneath all of that, you know the drinking, the pills, or the powder has stopped being something you control.
Disappearing for thirty days isn’t on the table. That doesn’t mean treatment is off the table.
Outpatient drug programs in the Portland metro have grown into a clinically serious option, with research showing intensive outpatient care works as well as inpatient treatment for most people who enter it 1. You keep your apartment, your paycheck, and most of your week. You add structured hours, real clinical work, and a plan for the parts of your life that got loud.
This guide is written for working adults in Portland and Milwaukie who are quietly weighing this decision, and for the spouses, partners, and HR contacts helping someone they care about. You’ll find what outpatient actually looks like week to week, how it sequences with detox and step-down care, how to protect your privacy and your license, and how to vet a local program without falling for amenity talk. No sales pitch. Just a clearer map.
What outpatient drug treatment actually looks like
The continuum: detox, PHP, IOP, and standard outpatient
Outpatient isn’t one thing. It’s a ladder, and where you start depends on what your body and your life are doing right now.
Oregon’s behavioral health framework recognizes several levels of substance use disorder care, including outpatient and intensive outpatient services 6. Knowing the rungs helps you ask for the right one instead of getting handed whatever a clinic happens to sell.
- Medical detox
- Comes first if your body is physically dependent on alcohol, benzodiazepines, or opioids. This is the medically supervised stretch, usually a few days to a week, where withdrawal is managed safely. For benzodiazepines and alcohol especially, skipping this step can be dangerous.
- Partial hospitalization (PHP)
- The most intensive outpatient level, usually around 20 or more hours per week of clinical programming, often five days a week during the day. You sleep at home. You spend most of your weekday hours in treatment. PHP fits people stepping down from detox who still need a lot of structure but don’t need a residential bed.
- Intensive outpatient (IOP)
- Typically runs 9 to 19 hours per week, often three evenings a week plus a weekend group. This is the level most working professionals land on, because it leaves room for a real job.
- Standard outpatient
- Under 9 hours per week, sometimes as little as one weekly group plus an individual session. It’s where you go after IOP, not usually where you start.
- Aftercare and alumni programming
- Wraps around all of it: monthly check-ins, sober community, recovery coaching, relapse-prevention groups that keep going for a year or more.
Most people don’t pick one rung and stay there. You step down as you stabilize. The continuum is the point.
A typical week: evening tracks, telehealth, and group sessions
Here’s what an IOP week often looks like for someone working a full schedule in the Portland metro.
Three evenings a week, usually Monday, Wednesday, and Thursday, you show up to a group from roughly 5:30 to 8:30 p.m. You eat a quick dinner before or during. The group runs about three hours and mixes education, skills work, and process discussion. Topics cycle through cravings, triggers, sleep, relationships, communication, and the slow work of figuring out what your life looks like without the substance running it.
Once a week you meet one-on-one with a counselor for 50 to 60 minutes. Some programs do this in person; many offer telehealth so you can take the session from a home office or a parked car between meetings. Telehealth has become a real piece of outpatient care in Oregon, not a backup option.
You may also have a weekend group, often Saturday morning, that focuses on relapse prevention or family work. Some programs add a separate family or couples session every few weeks.
Drug testing is standard, usually random and frequent in the first months. It’s not punitive. It’s part of how the program protects your progress and gives your counselor real information.
Add it up: about 9 to 12 hours of structured time, plus whatever recovery support you build around it, like a 12-step meeting, SMART Recovery, or a peer group. Your mornings stay yours. Your workday stays yours. The evening is the trade.
It’s a lot. It’s also finite. Most IOPs run 8 to 12 weeks at full intensity before stepping down.
Medication options inside outpatient care
If your situation involves opioids or alcohol, medication is probably part of the conversation, and you should know that going in.
The Oregon Health Authority regulates opioid treatment programs that prescribe and administer FDA-approved medications for opioid use disorder, including buprenorphine, methadone, and naltrexone, integrated with counseling 4. In plain terms: medication that reduces cravings and blocks the worst of withdrawal, paired with the therapy work you’re already doing in group and individual sessions. This combination is often called medication-assisted treatment, or MAT.
For alcohol, the common options are naltrexone (oral or a monthly injection), acamprosate, and disulfiram. Each works differently. Naltrexone dulls the reward; acamprosate steadies the nervous system in early recovery; disulfiram makes drinking physically unpleasant.
Some programs prescribe directly. Others coordinate with your primary care doctor or a partner clinic. Ask early how a program handles this, because it changes how your week looks and how supported you’ll feel between sessions.
If a program tells you medication is off the table on principle, that’s information. You’re allowed to want every evidence-based tool available to you.
Is outpatient enough, or do you need residential first?
What the research says about IOP outcomes
Here’s the honest answer most clinics won’t lead with: for most people who walk in the door, intensive outpatient gets you to the same place residential does.
A peer-reviewed assessment of intensive outpatient programs across multiple settings concluded that IOPs are as effective as inpatient treatment for most individuals with substance use disorders 1. That’s a national finding from trials comparing the two settings on outcomes like abstinence, retention, and follow-up functioning. It’s not a guarantee, and it’s not every person. It is the strongest evidence base you have for choosing outpatient without feeling like you’re choosing the lesser option.
What that means in plain terms: if you’re a working professional weighing whether outpatient is real treatment or just a compromise, the research says it’s real treatment. The structure, the group work, the medication options, the accountability of regular drug testing and weekly individual sessions—those mechanics do the work. A residential bed gives you 24-hour supervision and removal from your environment. Both matter for some people. Neither is automatically superior.
When residential or PHP is the safer entry point
That said, outpatient isn’t the right starting point for everyone, and it’s worth being honest with yourself about which side of the line you’re on.
An Oregon study comparing treatment settings for opioid use disorder found that outcomes vary by setting, with residential care showing advantages for some people with more severe presentations 5. Severity isn’t only about how much you use. It’s about whether your home environment is actively dangerous to your recovery, whether you’ve tried outpatient before and couldn’t hold it, whether you have unmanaged psychiatric symptoms, or whether your physical dependence on alcohol or benzodiazepines makes withdrawal a medical event.
If you’re using daily, drinking heavily every night, or relying on benzodiazepines, start with medical detox. From there, PHP gives you most of the structure of residential without the bed. If your home is stable, your job is flexible enough for evenings, and your physical dependence is mild or already managed, IOP is a reasonable first stop. A good intake assessment will tell you which rung fits. Ask for that conversation.
Why timing matters for Portland-area access right now
Two things are true about getting into outpatient treatment in the Portland metro right now, and they pull in opposite directions.
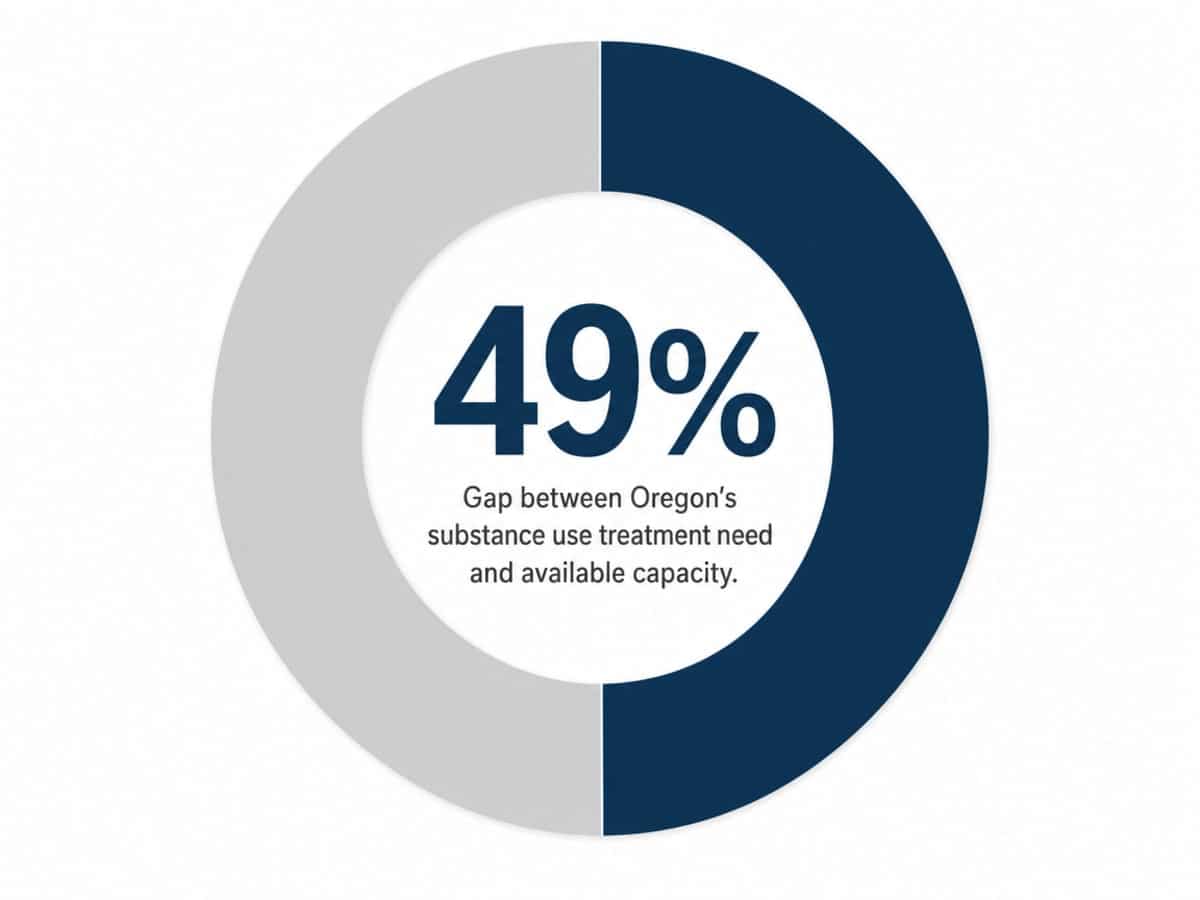
The first: Oregon’s substance use disorder treatment system has a 49% gap between the services Oregonians need and the capacity available to deliver them, according to the state’s own inventory and gap analysis 7. That’s a statewide unmet-need estimate, not a Portland-only figure, but Multnomah County sits inside it. In practical terms, calling around can mean waitlists, intake assessments scheduled two or three weeks out, and evening IOP cohorts that fill before you finish thinking it over.
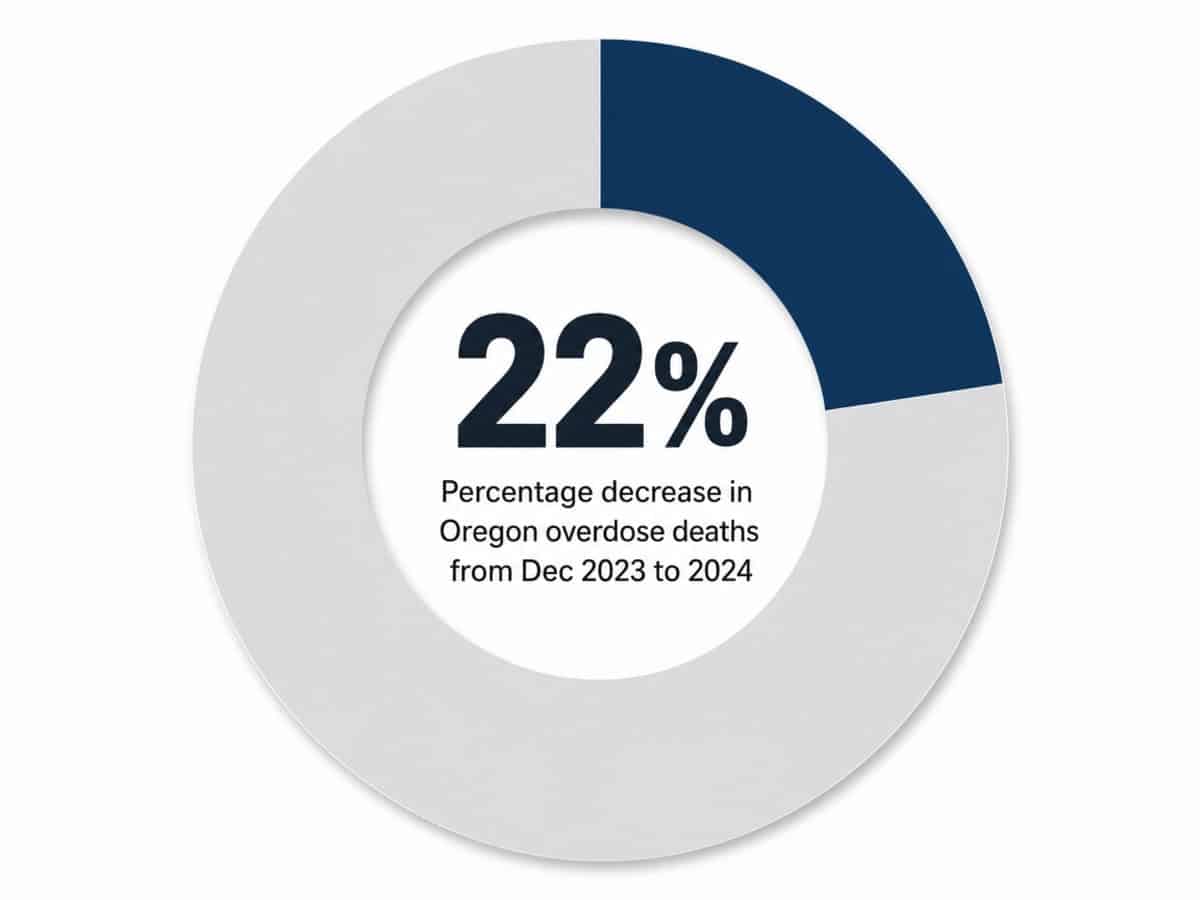
The second: things are actually moving in the right direction. Oregon’s overdose deaths dropped 22% between December 2023 and December 2024 based on CDC data, a shift state officials link to expanded treatment access and harm-reduction efforts 10. More people are getting into care. More people are staying alive long enough to do the work.
Both of these matter for you. The gap means you should not assume you can pick up the phone Monday and start Tuesday. The downward overdose trend means the system is responding, and the door is more open than it was two years ago.
Waiting another month to feel ready usually just means waiting another month plus the wait time you would have already worked through.
Protecting your career, license, and privacy
Confidentiality, HR, and licensure boards
The fear is rational. You’re not paranoid for asking who finds out.
Here’s the baseline: federal regulations under 42 CFR Part 2 give substance use treatment records stronger privacy protection than ordinary medical records. A program cannot release the fact that you’re enrolled, much less your treatment notes, without your written consent. That’s true whether your employer asks, your insurance asks, or a family member asks. You sign releases for what you want shared. Nothing else moves.
For most working professionals, that means HR never has to know. You use your insurance, the claim is processed like any other behavioral health claim, and your employer sees nothing about diagnosis or service type beyond what any benefits administrator already sees, which is usually nothing.
If you’re worried about an Employee Assistance Program contact, you can self-refer to a community-based outpatient program directly through Oregon’s certified provider network without going through your EAP at all 8. The EAP is a resource. It’s not a requirement.
Licensure boards are the more delicate piece. Oregon’s medical, nursing, legal, and pilot boards each have their own self-reporting rules, and they vary on whether voluntary treatment must be disclosed. Talk to a licensure attorney before you assume the worst. Many boards actually treat self-initiated treatment as a protective factor, not a red flag.
Scheduling around PTO, court calendars, and shift work
The schedule is the part most people quietly worry will be the dealbreaker. It usually isn’t.
Evening IOP tracks exist precisely because the people who need them work during the day. A 5:30 to 8:30 p.m. group means you can finish a workday in the Pearl, downtown, or out in Beaverton, grab dinner, and make the session without taking PTO. Telehealth fills the gaps for individual sessions when you’re traveling, in trial, or pulling a long shift.
If you’re a tradesperson, nurse, or anyone on rotating shifts, ask up front whether the program offers multiple weekly cohorts you can move between. Some do. The good ones build the schedule around adult lives, not the other way around.
For court-mandated treatment, including DUII cases, programs that work routinely with Oregon courts already know how to document attendance, complete required assessments, and communicate with your attorney or probation officer on a defined release. You don’t have to coordinate it yourself.
Block the recurring evenings on your calendar as a personal appointment. That’s all most colleagues need to see.
How to vet a Portland outpatient program
Certification, MAT integration, and outcome measurement
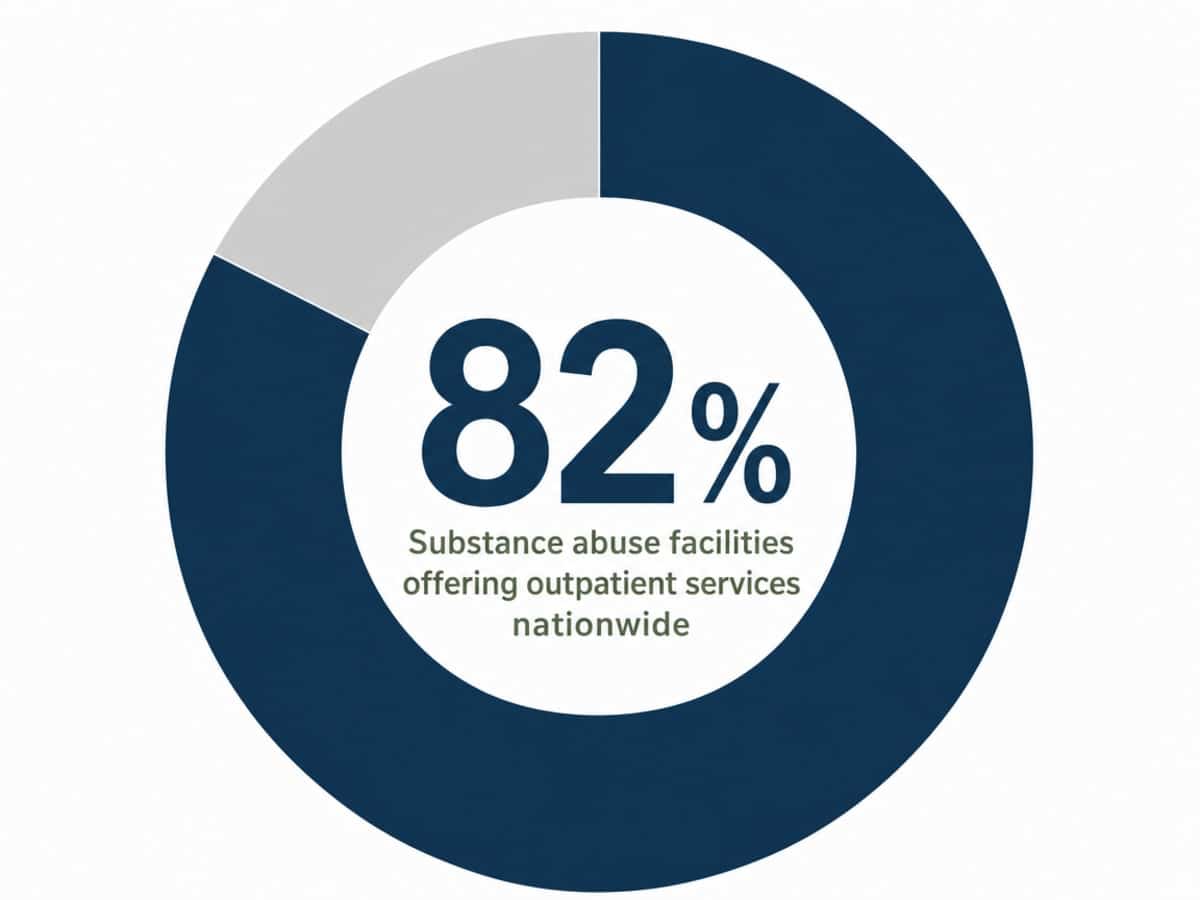
Outpatient treatment is everywhere. Nationally, 82% of substance abuse treatment facilities offer some form of outpatient service, according to SAMHSA’s National Survey of Substance Abuse Treatment Services 12. That number is good news and a warning at the same time. Good news because access exists. Warning because availability isn’t quality, and the program down the street from your office may or may not be one you’d want your sister enrolled in.
Three things separate a serious program from a storefront.
Certification. Oregon certifies behavioral health outpatient programs that treat substance use disorders, including IOPs, through the Oregon Health Authority 8. Ask any program for their OHA certification status. A real one will answer in a sentence. If the question makes the intake coordinator nervous, keep calling.
MAT integration. If opioids or alcohol are part of your picture, ask whether the program prescribes medication on site, coordinates with a partner clinic, or expects you to find your own prescriber. The OHA-regulated framework allows medications like buprenorphine, methadone, and naltrexone alongside counseling 4. A program that integrates these makes your week simpler. A program that punts on medication adds a job to your already-full plate.
Outcome measurement. This is the quiet differentiator. Ask, plainly: how do you know your program works? A serious provider tracks completion rates, abstinence at follow-up, and patient-reported functioning, and can talk about their numbers. A weaker one will tell you about their staff’s experience or their building. Experience matters. So does evidence that the work pays off.
Insurance, OHP, and what coverage usually looks like
Most commercial insurance plans in Oregon cover outpatient substance use treatment, including IOP and PHP levels, as part of behavioral health benefits. Your plan will typically have a copay or coinsurance per visit, and many plans require prior authorization for IOP and PHP. The intake team at any reputable program runs your benefits before you start, so you know the number before you commit.
Oregon Health Plan (OHP, the state’s Medicaid program) covers outpatient and intensive outpatient SUD services under OHA’s behavioral health rules 13. Not every private outpatient program accepts OHP, though. Some do, some don’t. Ask directly on the first call. If a program doesn’t take your coverage, ask them to refer you to one that does, or use Oregon’s Substance Use Disorder Provider Directory to find a fit 9.
Don’t let cost paralyze you into doing nothing. Get the benefits check. Then decide.
Questions to ask on the first call
Keep this list on your phone. Twenty minutes on the first call saves you weeks of regret.
- Are you OHA-certified for outpatient SUD services?
- What levels of care do you offer, and how do you decide which one fits me?
- Do you have an evening IOP track, and which nights does it run?
- Do you prescribe medication on site, or coordinate it externally?
- How do you handle telehealth for individual sessions?
- What’s your typical wait time from assessment to start date?
- Do you accept my insurance, and what will I owe per week?
- How do you measure outcomes, and what do yours look like?
- Have you worked with professionals who have licensure considerations?
If a program answers these clearly, you’re talking to the right kind of place. If they dodge, keep dialing.
Making the first move
The hardest part is usually the first phone call. Not the treatment. Not the schedule. The call.
Here’s a softer version of it: you don’t have to commit to anything to get an intake assessment. You’re booking a conversation. A clinician asks questions, listens to what’s actually going on, and tells you which level of care fits, whether that’s detox first, PHP, IOP, or something lighter. You can say yes. You can say not yet. You can ask for a second opinion. Nothing on that call obligates you to enroll.
If you’re not sure where to start, Oregon’s Substance Use Disorder Provider Directory lists certified outpatient programs across the Portland metro 9. Pick two or three. Call them this week. Ask the questions from the checklist above.
Pacific Crest Trail Detox is one local option built around the continuum this guide describes. Whichever door you walk through, walk through one. You’re allowed to want your life back.
Check Your Coverage for Outpatient Drug Care
See if your insurance supports discreet outpatient treatment in Portland.
Frequently Asked Questions
How many hours per week does an outpatient drug program in Portland require?
It depends on the level. Intensive outpatient (IOP) usually runs 9 to 19 hours a week, often three evening groups plus a weekly individual session. Partial hospitalization (PHP) runs around 20+ hours a week. Standard outpatient is under 9 hours. Oregon’s behavioral health framework recognizes all three levels 6.
Can I keep working full-time while in an outpatient program?
Yes, and that’s the point. Evening IOP tracks (typically 5:30 to 8:30 p.m.) are built around a normal workday. Telehealth often covers individual sessions when you travel or pull a long shift. Most working professionals in the Portland metro complete IOP without taking PTO. PHP is harder to fit around full-time work and usually requires schedule flexibility.
Will my employer or licensing board find out I’m in treatment?
Federal regulations under 42 CFR Part 2 protect substance use treatment records. A program cannot release your enrollment or notes without written consent. Insurance claims process as standard behavioral health, not as treatment-specific. Licensure boards have separate self-reporting rules that vary by profession, so talk to a licensure attorney before assuming disclosure is required.
Do I need to complete detox before starting an outpatient program?
Only if you’re physically dependent on alcohol, benzodiazepines, or opioids. For these substances, withdrawal can be medically serious and benzodiazepine or alcohol withdrawal can be life-threatening. Medical detox usually runs a few days to a week. If your use is mild or already managed, intake assessments often route you straight into IOP. Ask for the assessment first.
Does insurance or the Oregon Health Plan cover outpatient drug treatment?
Most commercial insurance plans in Oregon cover IOP and PHP under behavioral health benefits, often with a copay and prior authorization. The Oregon Health Plan covers outpatient and intensive outpatient SUD services under OHA rules 13. Not every program accepts OHP, so ask on the first call. The state’s provider directory can help you find a fit 9.
Is outpatient treatment effective for opioid or alcohol use disorder?
For most people, yes. A peer-reviewed assessment found IOPs as effective as inpatient treatment for most individuals across multiple settings 1. Medication options like buprenorphine, methadone, and naltrexone can be integrated alongside counseling under OHA-regulated programs 4. People with severe presentations or unstable home environments may do better starting with residential or PHP 5.
References
- Substance Abuse Intensive Outpatient Programs: Assessing the …. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- [PDF] Oregon Substance Use Disorder Services Inventory and Gap Analysis. https://www.oregon.gov/oha/HSD/AMH/DataReports/SUD-Gap-Analysis-Inventory-Report.pdf
- [PDF] Oregon SUD System Assessments and Analyses 2020-25. https://www.oregon.gov/adpc/Committee%20Resources/Summary%20of%20Assessments%20and%20Gaps%20Analyses%202020-25.pdf
- Oregon Health Authority : Medication-Assisted Treatment for Opioid …. https://www.oregon.gov/oha/hsd/amh/pages/mat.aspx
- Association between treatment setting and outcomes among oregon …. https://pmc.ncbi.nlm.nih.gov/articles/PMC9389731/
- [PDF] Substance Use Disorder Integration Report – Oregon.gov. https://www.oregon.gov/oha/HSD/AMH/DataReports/SUD-Integration-Report.pdf
- Oregon Substance Use Disorder Services Inventory and Gap Analysis. https://www.oregon.gov/adpc/pages/gap-analysis.aspx
- Behavioral Health Outpatient Treatment Programs … – Oregon.gov. https://www.oregon.gov/oha/hsd/amh-lc/pages/op.aspx
- Addiction Services : Behavioral Health Division : State of Oregon. https://www.oregon.gov/oha/hsd/amh/pages/addictions.aspx
- Oregon overdose deaths are down, CDC data shows. https://www.oregon.gov/oha/erd/pages/oregon-overdose-deaths-are-down-cdc-data-shows.aspx
- Multnomah County, Oregon – U.S. Census Bureau QuickFacts. https://www.census.gov/quickfacts/fact/table/multnomahcountyoregon/PST045224
- National Survey of Substance Abuse Treatment Services (N-SSATS). https://www.samhsa.gov/data/sites/default/files/reports/rpt35313/2020_NSSATS_FINAL.pdf
- Behavioral Health Services Rules and Guidelines … – Oregon.gov. https://www.oregon.gov/oha/hsd/ohp/pages/policy-bhs.aspx


