
Key Takeaways
- Alcohol withdrawal unfolds in a predictable arc: tremors and anxiety by 12 hours, peak seizure risk at 24 to 48 hours, and delirium tremens opening after 48 hours.9
- Heavy daily drinkers face real danger quitting cold turkey at home, since withdrawal seizures and DTs are medical emergencies that need supervised care and monitoring.2
- Benzodiazepines remain first-line because they roughly triple the odds of therapeutic success within two days, and fixed-schedule diazepam is the only agent shown to reduce DT cases.7,8
- Detox is step one, not the finish line, and guidelines are explicit that withdrawal care must link to ongoing treatment for gains to hold.3
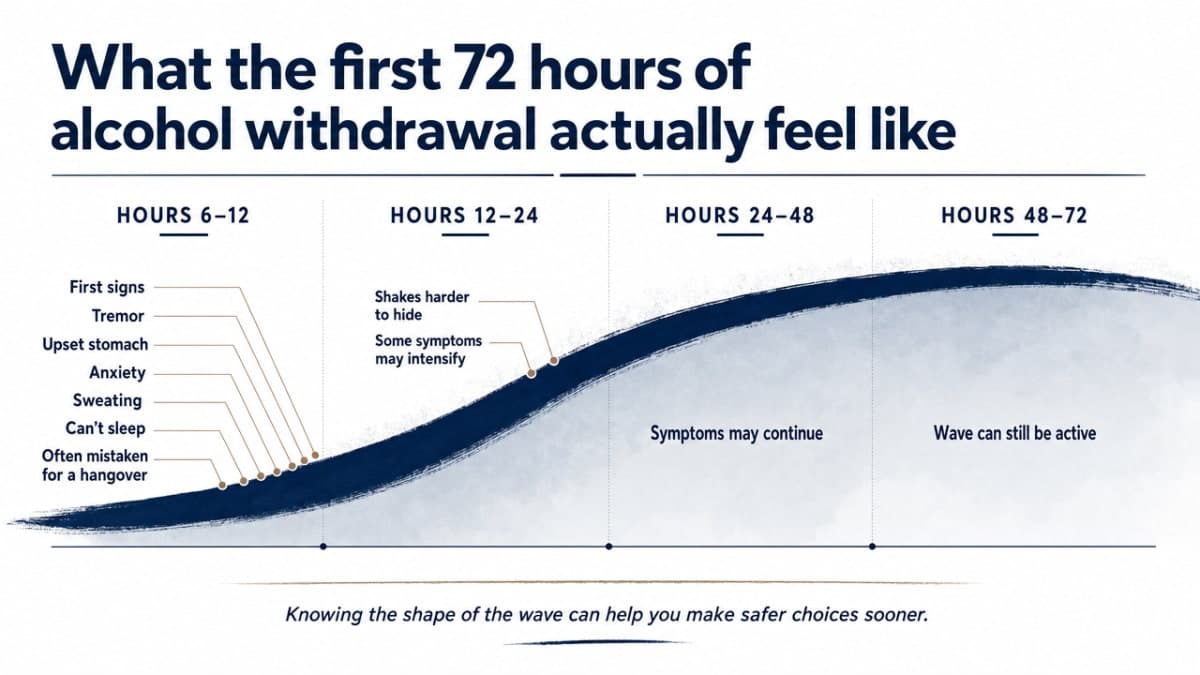
What the first 72 hours of alcohol withdrawal actually feel like
If you’re reading this after a rough morning of shakes, a racing heart, or a sleepless night, take a breath. You’re already doing something important by trying to understand what your body is going through. Alcohol withdrawal guideline isn’t a single event. It’s a wave that builds over three days, and knowing the shape of that wave can help you make safer choices, sooner.2,9
Hours 6 to 12. The first signs usually show up within half a day of your last drink. Your hands may tremble. Your stomach turns. Anxiety creeps in, sweat beads on your forehead, and sleep feels impossible. Many people mistake this for a bad hangover and pour another drink to make it stop. That’s the trap: the symptoms mean your nervous system is already firing without the brake alcohol used to provide.
Hours 12 to 24. The shakes get harder to hide. Some people begin to see or hear things that aren’t there, sometimes shadows, sometimes voices. This is frightening but not the most dangerous phase yet.
Hours 24 to 48. This is when the risk of a withdrawal seizure peaks. Seizures can happen without warning, even in people who’ve never had one before.
Hours 48 to 72 and beyond. The window for delirium tremens opens. DTs bring severe confusion, fever, a pounding heartbeat, and dangerous swings in blood pressure. It’s a medical emergency, and it needs hospital-level care.
You don’t have to guess where you are on this map alone. That’s what supervised care is for.
Why quitting cold turkey at home can be dangerous
If you’ve been drinking heavily every day for weeks, months, or years, your brain has adjusted to alcohol as a constant. Take it away suddenly and the nervous system rebounds hard. That rebound is what makes home detox from heavy alcohol use different from quitting most other substances. It isn’t a matter of willpower. It’s biology.
The specific risks are worth knowing by name, not so you’ll panic, but so you can make an informed call.
Seizures. A withdrawal seizure can strike someone with no history of epilepsy. It can happen while you’re driving, showering, or sleeping alone. Guidelines built for hospitals stress catching withdrawal early and starting medication before symptoms get severe, because prevention is far safer than reaction.9
Delirium tremens. DTs are not just “bad shakes.” They involve severe confusion, high fever, and dangerous shifts in heart rate and blood pressure. The medical literature is direct: DTs need to be managed as a medical emergency, ideally in an inpatient or ICU setting. At home, without IV access and monitoring, the mortality risk climbs.2
Aspiration and cardiac events. A person seizing or deeply confused can vomit and choke. Blood pressure can spike or crash. These are the kinds of complications a family member simply cannot manage from a bedroom.
The trap of “just one more drink.” When symptoms hit hard, many people drink again to make them stop. That works for an hour, then the cycle repeats, often worse. You’re not weak for this. You’re caught in a loop your nervous system built, and breaking it safely takes support.
How clinicians assess withdrawal severity, in plain language
CIWA-Ar: what a nurse is really watching for
You may hear a nurse mention “CIWA” during intake and wonder what that means for you. CIWA-Ar is a short checklist a nurse uses to measure how strongly your body is reacting to the lack of alcohol. It stands for the Clinical Institute Withdrawal Assessment for Alcohol, revised. Think of it as a set of gentle questions and quick observations, not a test you can pass or fail.
Every few hours, someone sits with you and checks ten things: how much your hands shake, whether you’re sweating, if your stomach feels sick, how your head feels, whether sounds seem too loud, whether lights bother your eyes, whether you feel bugs on your skin or see or hear things that aren’t there, how anxious or restless you feel, and whether you know where you are and what day it is. Each item gets a small score. Added up, they give a number.
That number tells the team how much medication you need and how often to come back. A low score means keep watching. A rising score means it’s time to give more support before things get worse. Guidelines used in hospitals rely on tools like CIWA-Ar to catch withdrawal early and adjust doses safely, which is exactly why the check-ins happen so often. The regular knock at your door isn’t intrusion. It’s the safety net doing its job.9,11
Risk factors that raise the stakes
Not everyone going through alcohol withdrawal faces the same danger. A good intake nurse will ask questions that sound personal because your history changes the plan. Be honest here. It helps them keep you safe.
Certain histories bump you into a higher-risk group. A past withdrawal seizure, even one, means your brain has already crossed that line once and can do it again more easily. A previous episode of delirium tremens is a strong warning sign. Daily heavy drinking, drinking to stop the morning shakes, older age, poor nutrition, other medical conditions like liver or heart disease, and using benzodiazepines or opioids alongside alcohol all raise the stakes.9
None of this is meant to scare you. It’s meant to match your care to your body. If any of those apply to you, a residential medical detox with round-the-clock monitoring is a safer starting point than trying to ride it out at home. Tell the team everything, including the drink you didn’t want to admit to. They’ve heard it before, and the more they know, the better they can protect you.
The medication question: benzodiazepines, gabapentin, and what the evidence says
Why benzodiazepines are first-line
If the idea of taking a medication during detox makes you uneasy, you’re not alone. A lot of people wonder if they’re just swapping one drug for another. The honest answer is: no, and here’s why the medical world lands on the same medication family again and again.
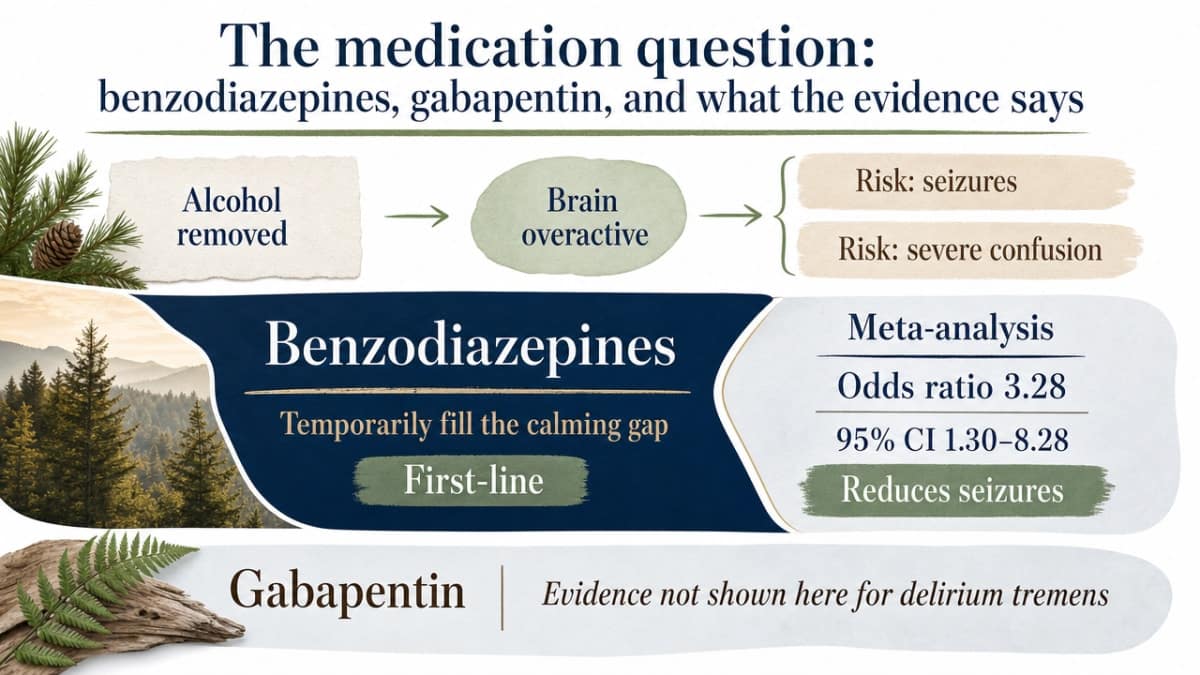
Alcohol quiets a system in your brain that keeps you calm. When alcohol suddenly disappears, that quieting effect is gone, and the brain becomes overactive. Benzodiazepines gently take over that calming job for a few days while your brain resets. Without something to fill that gap, the overactivity can spill into seizures or severe confusion.
The evidence supporting this is not new or thin. A foundational meta-analysis found that people treated with benzodiazepines had an odds ratio of 3.28 (95% CI 1.30–8.28) for therapeutic success within two days of acute alcohol withdrawal treatment, compared to placebo. In plain English: those given a benzodiazepine were about three times more likely to be in good shape within two days than those given nothing.7
A separate Cochrane-based summary reached a similar conclusion: benzodiazepines protect against withdrawal seizures better than placebo. That is the reason nurses hand you a small dose instead of asking you to tough it out. It’s not to sedate you into a fog. It’s to keep your brain from lighting up in ways that can hurt you.10
Which specific medications reduce seizures and DTs
Not every benzodiazepine, and not every dosing style, does the same job. This matters because the two things you most want to avoid, seizures and delirium tremens, respond differently to different medications.
The most complete picture comes from a 2022 network meta-analysis that pulled together 149 randomized trials. The researchers compared many different drugs used for alcohol withdrawal and asked two direct questions: which ones prevent seizures, and which ones prevent DTs?8
For seizures, five agents beat placebo: fixed-schedule diazepam (brand name Valium), lorazepam (Ativan), chlordiazepoxide (Librium), chlormethiazole, and divalproex. The first three are benzodiazepines, which is why you’ll hear those names most often in a detox setting. Divalproex is an anticonvulsant, and chlormethiazole is used more in Europe than in the U.S.8
For delirium tremens, the picture narrowed sharply. Out of every medication studied across those 149 trials, only fixed-schedule diazepam reduced the number of DT cases compared to placebo. That is a striking finding, and it’s part of why an experienced medical team may choose a scheduled diazepam approach for someone whose history suggests real DT risk (a past DT episode, prior withdrawal seizures, long heavy daily drinking).8
The takeaway isn’t that one drug is magic and the others don’t work. It’s that the choice of medication is a clinical decision matched to your risk. When a nurse asks about your drinking history, past withdrawals, and other health conditions, that information is what tells the team which medication and which schedule fits you best.
Symptom-triggered vs fixed-schedule dosing
You may hear two phrases float around during intake: “symptom-triggered” and “fixed-schedule.” Both describe how medication gets to you, and knowing the difference helps you ask the right questions.8
- Symptom-triggered
- means you get a dose when your CIWA score rises to a set number. If you’re doing well, you get less medication. If symptoms flare, the dose comes quickly. It works well for people at low to moderate risk because it avoids over-sedation.
- Fixed-schedule
- means doses are given at set times, whether or not symptoms have spiked, with extra doses available if needed. This approach is often chosen for people with a higher risk of severe withdrawal, since it keeps a steady calming effect in the body and, based on the network meta-analysis findings above, is the only approach shown to reduce actual DT cases.
Neither approach is one-size-fits-all. A good detox team decides based on your history and adjusts if the plan isn’t working. If you’re curious, ask which method they’re using and why. You have every right to understand what’s going into your body.
Where gabapentin fits (and where it doesn’t)
Gabapentin comes up often in newer conversations about alcohol withdrawal, and it’s fair to ask about. It’s a nerve-calming medication that some clinicians use as an add-on or, in milder cases, as an alternative to benzodiazepines.
Research has taken it seriously. A clinical trial compared gabapentin head-to-head with lorazepam, a standard benzodiazepine, to see how it holds up for withdrawal symptoms. A separate hospital study looked at what happens when gabapentin is added to a benzodiazepine plan. The honest read of that literature: gabapentin has a role, but benzodiazepines remain the gold standard, especially when the risk of seizures or DTs is real.4,5
What this means for you: if a clinician suggests gabapentin as part of your plan, it’s not a downgrade. It may be a reasonable choice for milder withdrawal, or a supportive add-on. But if your history includes past seizures, DTs, or heavy long-term drinking, don’t be surprised if a benzodiazepine is still the core of your care. That isn’t outdated thinking. It’s the medication with the strongest track record for the outcomes that matter most.
Supportive care: thiamine, fluids, sleep, and the room around you
Medication is the headline, but it’s only part of what keeps you safe during detox. The quieter parts of care matter just as much, and they’re worth knowing about so you understand why the team is fussing over things that seem small.6
Thiamine (vitamin B1). Heavy drinking depletes this vitamin, and running low on it can cause a serious brain condition called Wernicke-Korsakoff syndrome. Systematic reviews of alcohol withdrawal care specifically call out thiamine as a routine part of supportive treatment for heavy drinkers coming off alcohol. You may get it as a pill or a shot early in your stay. It’s not optional in a good protocol. It’s a small step that prevents a big problem.
Fluids and food. Many people arrive at detox dehydrated, undereating, and low on electrolytes like potassium and magnesium. Nurses will check your labs, push water, and offer simple foods your stomach can handle. If eating feels impossible the first day, that’s normal. Broth, crackers, and small bites come first.
Sleep. The first two nights are often the worst. You may not sleep much. The team plans for this and can help take the edge off so your body can rest and reset.
The room itself. A quiet, dim, familiar-feeling space lowers the nervous system’s baseline. Structured protocols expect regular vital-sign checks and gentle observation, not bright lights and beeping machines 11. A home-like setting isn’t just a nicer backdrop. It’s part of the calming.
Matching the person to the right level of care
Outpatient, residential medical detox, or hospital
Not everyone needs the same setting to get through withdrawal safely. The right level of care depends on how heavily you’ve been drinking, what your body has done during past attempts to stop, and what other health conditions are in the picture. National practice guidelines put it plainly: the setting should match the severity and medical risk, not the other way around.2,11,12
Outpatient detox can be reasonable for someone with mild symptoms, no history of seizures or DTs, stable health, and a sober, supportive person at home. You check in with a clinic, get medication, and return for daily monitoring. It works when the risk is genuinely low.
Residential medical detox is the middle ground, and it fits most people who’ve been drinking heavily every day, who’ve had shakes in the morning, or who’ve tried to quit before and slipped back. You get 24-hour nursing, scheduled CIWA-Ar checks, medication delivered on the schedule your body needs, thiamine, fluids, and a quiet room to rest in. It’s the setting built for the population most guidelines call “moderate risk.”
Hospital-based care is for the highest risk: active DTs, seizure activity, serious heart or liver disease, or symptoms that a residential program can’t safely manage. Say yes to it when it’s offered. It isn’t failure. It’s the right room for the moment.
When a residential detox transfers you to a hospital
Families sometimes worry that a transfer means something went wrong. It doesn’t. A good residential program has clear thresholds written into its protocols, and hitting one of them means the team is doing exactly what they promised: keeping you safe by moving you to the right level of care.11
The signs that trigger a hospital transfer are specific. A withdrawal seizure, even a brief one. Signs of delirium tremens, which is treated as a medical emergency and typically needs inpatient or ICU care. Vital signs that won’t settle despite adequate medication, like a heart rate that stays dangerously high or blood pressure that spikes or drops. A CIWA-Ar score that keeps climbing after appropriate dosing. Serious dehydration, chest pain, breathing trouble, or a mental status that changes fast.2,9
Here’s what to know as a family member: the ambulance ride is the safety net, not the alarm. The residential team stays in touch with the hospital, and once you’re stable, you can often come back to finish detox and step into the next phase of care. Ask the intake nurse to walk you through the transfer criteria on day one. Knowing the plan before you need it is one of the calmest things you can do.
What a home-like medical detox looks like in practice
A residential medical detox that feels more like a house than a hospital isn’t just cosmetic. It’s a deliberate choice about what helps a nervous system settle. You still get the same evidence-based care that a good hospital protocol offers, just without the fluorescent lights and the roommate on the other side of a curtain.
Here’s what a day actually looks like. You wake up in a real bed. A nurse comes by for a CIWA-Ar check-in and a vital-sign reading, on the schedule your risk level calls for. Medication is given on the plan chosen for you, whether that’s symptom-triggered or fixed-schedule. Thiamine, fluids, and food show up as part of the routine, not as an afterthought. Between check-ins, you can rest, take a shower, sit outside, or talk with someone who’s been where you are.6
Group time and one-on-one conversations start gently, when you’re ready. Nobody expects you to process your whole life on day two. What matters is that the structured protocol behind the calm surface, the vital signs, the scoring, the medication schedule, the escalation criteria, is running the whole time. Safety underneath. Warmth on top.11
Detox is step one, not the finish line
Getting through the first week is a real win. Your body is settling, your sleep is coming back in patches, and the fog is starting to lift. Celebrate that. It took courage to walk in the door.
What comes next looks different for everyone. Some people step into a partial hospitalization program during the day and sleep at home. Others move into an intensive outpatient schedule a few evenings a week. Group work, one-on-one counseling, family sessions, and support for co-occurring anxiety, depression, or trauma are often part of the plan. If you need help finding options in your area, SAMHSA’s free, confidential helpline is available around the clock. Pacific Crest Trail Detox is one place that carries people through that whole arc, from the first shaky day to the steady weeks that follow.14
Check If Your Detox Care Is Covered Today
Quickly find out if your insurance supports safe, supervised alcohol withdrawal care.
Frequently Asked Questions
Is it safe to detox from alcohol at home?
For light or occasional drinking, symptoms are usually mild. For heavy daily drinking, home detox can be dangerous. Withdrawal seizures and delirium tremens are medical emergencies that need inpatient care. If you drink daily, shake in the morning, or have withdrawn before, choose supervised care.2
How long does alcohol withdrawal last?
Early symptoms start 6 to 12 hours after your last drink. Seizure risk peaks between 24 and 48 hours, and the delirium tremens window opens around 48 to 72 hours and beyond. Most acute physical symptoms ease within 5 to 7 days, though sleep and mood take longer to settle.9
What medications are used during medical detox?
Benzodiazepines like diazepam, lorazepam, and chlordiazepoxide are first-line because they protect against seizures better than placebo. Thiamine (vitamin B1) is given to prevent a brain condition called Wernicke-Korsakoff syndrome. Fluids, electrolytes, and sleep support round out the plan. Gabapentin may be added in select cases, but benzodiazepines remain the standard.5,6,10
What are delirium tremens, and how dangerous are they?
Delirium tremens, or DTs, bring severe confusion, high fever, a racing heart, and dangerous blood pressure swings, usually 48 to 72 hours after the last drink. They’re treated as a medical emergency and typically need inpatient or ICU care. Fixed-schedule diazepam is the one medication shown to reduce incident DT cases.2,8
How do I know if I need residential detox instead of outpatient care?
Outpatient can work if your symptoms are mild, you have no history of seizures or DTs, your health is stable, and you have sober support at home. Residential detox is safer if you drink heavily daily, wake with shakes, have withdrawn before, or have other medical conditions. Guidelines match the setting to your risk.12
What happens after detox is finished?
Detox handles the acute physical piece, but withdrawal care should never stand alone. Guidelines are clear that it needs to link to ongoing treatment. Next steps often include partial hospitalization, intensive outpatient groups, one-on-one counseling, and support for co-occurring anxiety or depression. SAMHSA’s free helpline can point you to options.3,14
References
- Benzodiazepines for alcohol withdrawal. https://pubmed.ncbi.nlm.nih.gov/20238336/
- Delirium Tremens: Assessment and Management. https://pmc.ncbi.nlm.nih.gov/articles/PMC6286444/
- Withdrawal Management. https://www.ncbi.nlm.nih.gov/books/NBK310652/
- Comparing the Treatment of Alcohol Withdrawal Syndrome Using Gabapentin vs Lorazepam. https://clinicaltrials.gov/study/NCT00229125
- Impact of Gabapentin Adjunct use with Benzodiazepines for the Treatment of Alcohol Withdrawal in Hospitalized Patients. https://pmc.ncbi.nlm.nih.gov/articles/PMC6386428/
- Clinical Management of Alcohol Withdrawal: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC4085800/
- Meta-analysis of Benzodiazepine Use in the Treatment of Acute Alcohol Withdrawal. https://pmc.ncbi.nlm.nih.gov/articles/PMC1230110/
- Comparative Efficacy and Safety of Pharmacotherapies for Alcohol Withdrawal: A Systematic Review and Network Meta-analysis. https://pubmed.ncbi.nlm.nih.gov/35194860/
- Alcohol Withdrawal in Hospitalized Patients. https://www.ncbi.nlm.nih.gov/books/NBK604324/
- Benzodiazepines for Alcohol Withdrawal. https://odphp.health.gov/healthypeople/tools-action/browse-evidence-based-resources/benzodiazepines-alcohol-withdrawal
- Guidance on Medical Protocols for Withdrawal Management for OASAS Certified Programs. https://oasas.ny.gov/medical-protocols-withdrawal-management
- ASAM Clinical Practice Guideline on Alcohol Withdrawal Management Pocket Guide. https://www.samhsa.gov/resource/ebp/asam-clinical-practice-guideline-alcohol-withdrawal-management-pocket-guide
- The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management (PubMed Record). https://pubmed.ncbi.nlm.nih.gov/32511109/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline


