
Key Takeaways
- Treatment is a connected continuum, not a single decision—people enter at the level matching their needs and step up or down as those needs shift 16.
- Clinicians match care using the ASAM six dimensions: withdrawal risk, medical issues, mental health, readiness, relapse potential, and the safety of the home environment 3.
- Medications like buprenorphine, methadone, and naltrexone paired with behavioral therapy produce the strongest outcomes for opioid and alcohol use disorders 10, 1.
- What sustains recovery after a program ends—continuing care through IOP, peer support, family involvement, telehealth, and harm reduction tools—matters as much as the initial level of care 13, 14, 8.
Why the system feels like alphabet soup at 2 a.m.
You’ve been awake for hours. Maybe your adult child is asleep down the hall after a hard night, or maybe you don’t know where they are right now. Either way, you’ve opened another browser tab, and somewhere between PHP, IOP, MAT, and ASAM, the words have started to blur.
That feeling isn’t a sign you’re behind. It’s a reasonable response to a system that uses a lot of acronyms to describe what is, at its heart, a sequence of medical and human decisions.
Here’s the quiet truth most websites bury: substance use treatment isn’t one choice. It’s a connected set of options, sometimes called a continuum of care, where a person enters at the level that matches their needs and steps up or down as those needs change 16. Detox is one step. Therapy is another. Medication can be part of the picture. So can family support, peer support, and follow-up visits done over video.
Your job tonight is not to pick the perfect program. It’s to understand enough of the map to ask good questions when you call someone in the morning. This guide walks you through the substance abuse treatment models clinicians actually use, in the order they tend to consider them, with plain language and a little breathing room.
How clinicians actually decide: the ASAM six-dimension assessment
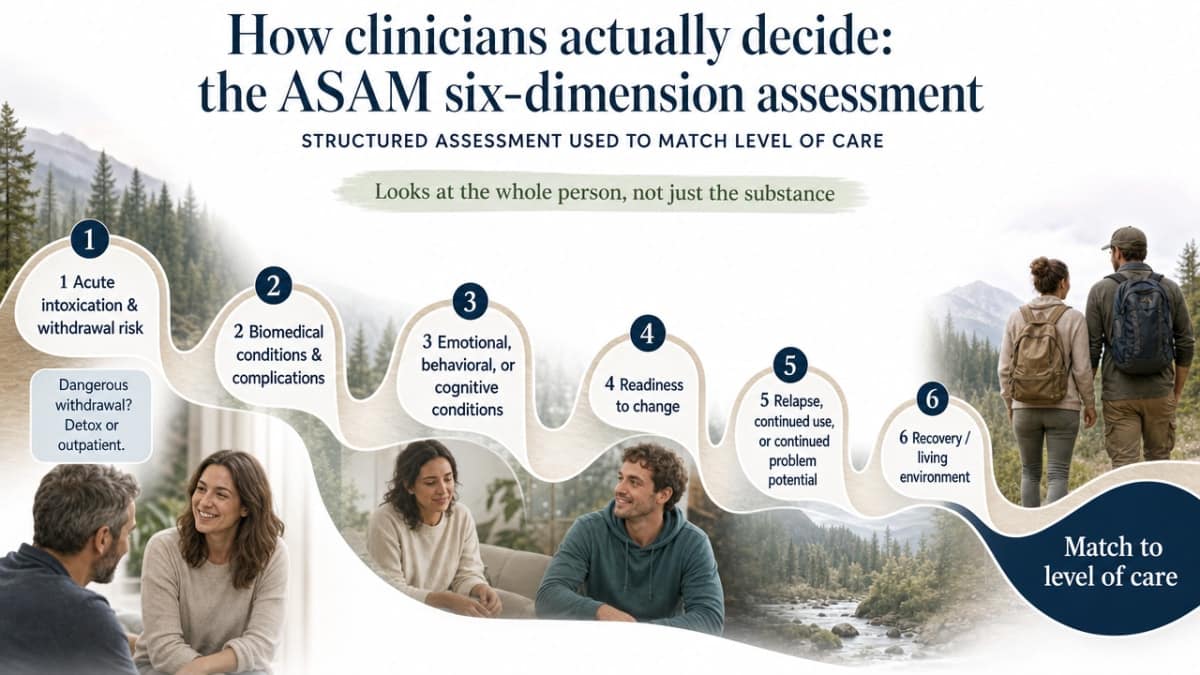
When you finally get someone on the phone at a treatment center, the intake clinician isn’t just asking what your adult child uses or how much. They’re working through a structured assessment most addiction specialists share in common, built around six dimensions developed by the American Society of Addiction Medicine 3. It’s the closest thing the field has to a shared language, and once you understand it, the rest of the acronyms start to make sense.
The six dimensions look at the whole person, not just the substance:
- Acute intoxication and withdrawal risk. Is your child likely to have a medically dangerous withdrawal from alcohol, benzodiazepines, or opioids? That single answer can determine whether the first stop is a medically supervised detox or an outpatient clinic.
- Biomedical conditions and complications. Are there other health issues — liver disease, pregnancy, chronic pain, recent injuries — that need monitoring alongside withdrawal?
- Emotional, behavioral, or cognitive conditions. Is depression, anxiety, PTSD, or another mental health condition part of the picture? Many adults with substance use disorders are carrying something else too 3.
- Readiness to change. Where is your child in their own thinking? Ready, ambivalent, or resistant? Clinicians don’t refuse care to people who aren’t “ready” — they meet them where they are.
- Relapse, continued use, or continued problem potential. How likely is a return to use without structure and support?
- Recovery environment. Is home a safe place to do the work, or are there people, pressures, or living conditions that will make outpatient care a setup for failure?
This is why two young adults using the same drug can land in completely different programs. One may go home each evening to a quiet apartment and a supportive partner; another may need residential care because the apartment isn’t safe yet. One has untreated PTSD that needs integrated mental health care; the other doesn’t. Federal guidelines for state Medicaid programs lean on this same framework when matching people to levels of care 2.
When you call a program, you can ask directly: How do you assess what level of care my child needs? A good answer will sound a lot like these six dimensions, even if the clinician doesn’t number them out loud. That’s a sign you’re talking to people who treat the whole person, not just the substance.
Medically supervised withdrawal: the safe first step
What detox does, and what it does not do
Detox is the medical bridge between active use and the rest of treatment. For some substances, that bridge is short and uncomfortable. For others — alcohol, benzodiazepines like Xanax or Klonopin, and sometimes opioids combined with other drugs — withdrawal can be medically dangerous, with seizures, severe blood pressure swings, or dehydration that need real monitoring 1.
What detox does: it gets your adult child through the acute withdrawal window safely. Clinicians use medications to ease cravings, calm the nervous system, and treat physical symptoms. Nurses watch vital signs. Someone is there at 3 a.m. when the worst hours hit.
What detox does not do: it doesn’t teach a person how to live without the substance. It doesn’t address the depression, trauma, or relationship pain that often sits underneath the use. NIDA is direct about this — medications and behavioral therapies together, sustained over time, produce the best outcomes 1. A clean week is a real win, and it’s the starting line, not the finish.
Hospital detox versus non-hospital medical detox in a home-like setting
Detox happens in two broad kinds of places. The first is inpatient hospitalization — a true medical floor with full hospital infrastructure, usually reserved for the most medically fragile cases or people who also need acute medical or psychiatric care 17. The second is non-hospital medical detox: a residential setting with 24-hour nursing and physician oversight, but without the beeping machines and shared rooms of a hospital ward.
The non-hospital model is sometimes called sub-acute detox. Your adult child sleeps in an actual bedroom. Meals are eaten at a table with other people in the same fight. Group therapy starts almost immediately, often within the first day or two, once medications have taken the edge off withdrawal 2. The clinical care is real — withdrawal medications, vital signs, physician check-ins — but the environment is built to feel less like a crisis and more like a place a person can begin to think again.
For many adults, that softer setting matters. It’s easier to stay through the hard middle days when the surroundings respect their dignity.
The levels of care, from 24/7 support to a weekly check-in
Residential treatment: living where the treatment happens
Residential treatment means your adult child sleeps, eats, and does their therapy work all in the same place, with staff on hand around the clock 17. It’s the most structured option short of a hospital, and it exists because some people simply cannot get sober in the environment they came from. The roommate is still using. The job is too stressful. The free hours in the afternoon are the dangerous ones.
A typical day in residential care isn’t a vacation. It’s structured group sessions, individual therapy, medical check-ins, meals together, and time for journaling, exercise, or rest. The point is to remove the cues and choices that have been driving the use, so the brain can start to reset and the harder therapy work becomes possible.
Length of stay varies. Some people stay a few weeks; others stay longer. NIDA’s research is consistent that shorter is rarely better — people who stay engaged in treatment for at least three months across the continuum tend to do best 1. Residential is often one chapter in that longer arc, not the whole book.
Partial hospitalization (PHP): clinic by day, home by night
PHP stands for partial hospitalization program. The name is a little misleading — no one is actually in a hospital. Think of it as a full clinical day, often five days a week, where your adult child shows up in the morning for group therapy, individual sessions, medication management, and skills work, then goes home or to sober housing at night 22.
It’s the level of care designed for people who need more than a few hours of therapy a week but don’t need someone watching them sleep. Maybe they’ve just stepped down from residential and aren’t quite ready for life with only evening support. Maybe they’re stable enough medically to go home, but their cravings are still loud and their coping skills are still new.
For a parent, PHP can feel like the first real exhale. You see them at dinner. You also know they spent the day doing the work.
Intensive outpatient (IOP) and standard outpatient: building life back around recovery
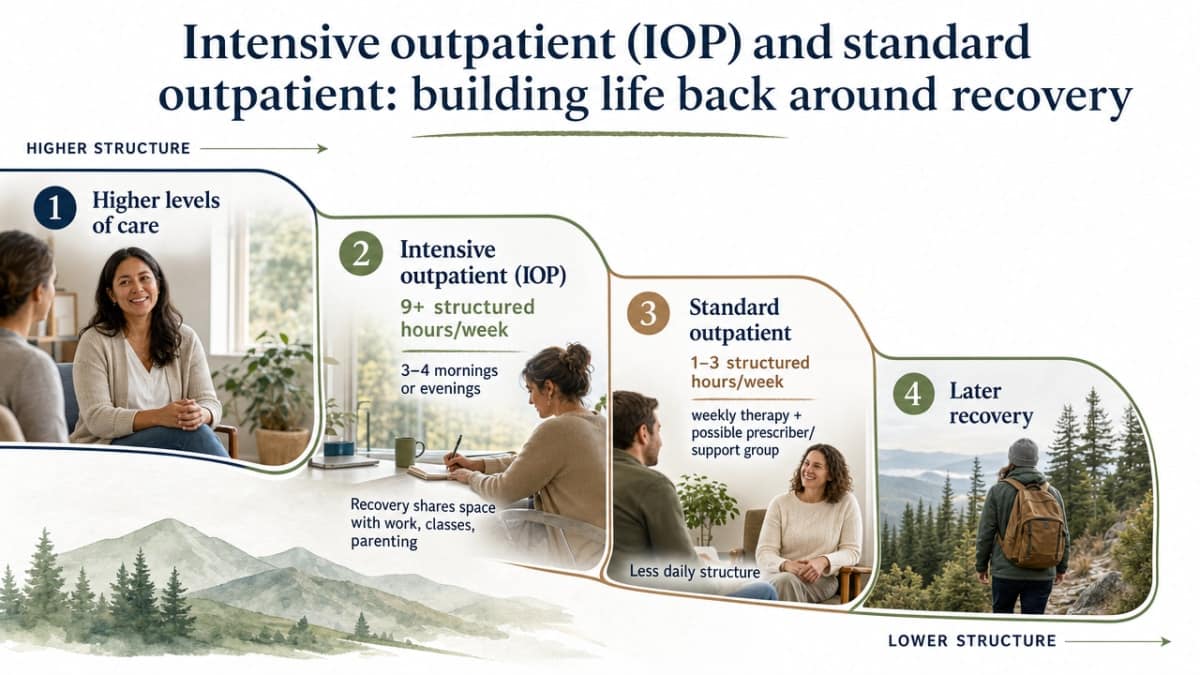
Intensive outpatient (IOP) is the next step down. Most IOPs run at least nine hours per week of structured group and individual treatment, usually spread across three or four evenings or mornings so people can hold a job, attend classes, or care for their own children 4. It’s where recovery starts to share space with the rest of life.
Standard outpatient is lighter still — usually a weekly therapy session, sometimes a check-in with a prescriber, sometimes a support group on top. It’s often where someone lands months into their recovery, when the daily structure of higher levels of care is no longer what they need.
To put the levels side by side, here is roughly what your adult child’s week looks like at each one:
- Standard outpatient: about 1 to 3 structured hours per week 22
- Intensive outpatient (IOP): at least 9 structured hours per week 4
- Partial hospitalization (PHP): roughly 20 or more structured hours per week, often a full clinical day 22
- Residential: 24-hour supervised care in the treatment setting 17
One finding that surprises a lot of parents: the research review on IOP concluded that intensive outpatient is as effective as inpatient treatment for many people, while letting them stay connected to home, work, and family 4. That doesn’t mean IOP is right for everyone — someone in acute withdrawal or living in an unsafe home isn’t a candidate for it. It does mean that if a clinician recommends IOP instead of a 30-day residential stay, they’re not cutting corners. They’re matching the level of care to what your child actually needs.
Medication for opioid and alcohol use disorder: a normal medical tool
If you’ve spent any time in recovery forums, you’ve probably run into the argument: is medication “real” recovery, or is it just swapping one drug for another? It’s worth saying clearly. The medications used to treat opioid and alcohol use disorder are FDA-approved, well-studied, and recommended by the same federal agencies that set the standards for the rest of addiction care 10.
For opioid use disorder, there are three main medications: methadone, buprenorphine, and naltrexone 18. Methadone and buprenorphine quiet the cravings and the physical drive to use, without producing the high that street opioids do. Naltrexone blocks the opioid receptor entirely, so using again doesn’t produce the same effect. For alcohol use disorder, naltrexone is also used, along with acamprosate and disulfiram, to reduce cravings or make drinking less rewarding.
Here’s the part that matters for your adult child’s day: a person on buprenorphine isn’t sedated. They go to work. They show up to therapy clearer-headed than they have been in years. The medication takes the constant pull of craving down to a manageable hum so the harder work — the counseling, the rebuilding, the rebuilding of trust — has room to happen 10.
The stigma around these medicines runs deep, sometimes inside families and sometimes inside well-meaning recovery communities 18. If a clinician recommends medication and you feel that old worry rise, it’s worth asking what they’ve seen in people who use it alongside therapy. The combination — medication plus behavioral treatment — is what the evidence supports, not one without the other 1.
The therapies that do the deeper work
Cognitive behavioral therapy and motivational approaches
Once the body steadies, the real conversation starts. Cognitive behavioral therapy, or CBT, is the one your adult child is most likely to encounter first. The work is practical: notice the situations, thoughts, and feelings that drive use, then build different responses to them. A counselor might walk through what happened the last time your child relapsed — the long Tuesday at work, the text from the wrong friend, the half-formed thought that one drink would help — and then practice what could go differently next time. Researchers reviewing CBT for substance use disorders found it works as a standalone treatment and as part of combined approaches 5.
Motivational approaches sit alongside CBT in most programs. Instead of arguing your child into change, the counselor draws out their own reasons for it 1. That matters when readiness is uneven, which it almost always is.
Integrated care for co-occurring depression, anxiety, or PTSD
For a lot of adults, the substance use isn’t the whole story. There’s also a depression that started in college, an anxiety that never quite quieted, a trauma no one ever named out loud. When mental health goes untreated, recovery tends to wobble. When it’s treated separately, in a different building by a different team that doesn’t talk to the first one, recovery wobbles too.
Integrated care means one team treats both conditions at the same time, in the same place, with everyone reading the same notes 6. SAMHSA recommends this approach for people with co-occurring disorders rather than treating each problem in isolation 19. In practice, that might look like your child seeing a psychiatrist for an antidepressant on Tuesday and a counselor for cravings on Wednesday — both knowing what the other adjusted, both working from the same plan.
If you’re asking one question at intake, ask this: how does the program handle mental health alongside substance use?
Trauma-informed care: what the phrase actually means
Trauma-informed care has become a phrase programs put on their websites. It can mean a lot, or it can mean very little. The framework SAMHSA actually describes is built on four actions: realize how widespread trauma is, recognize its signs in clients and staff, respond by weaving that knowledge into every part of the program, and actively resist re-traumatizing the people who walk in the door 20.
On the ground, it shows up in small choices. Doors that don’t lock people in unnecessarily. Staff who explain what’s about to happen before they do it. Group rules that protect choice and voice. SAMHSA points out that many people in substance use treatment carry trauma histories, and a program that ignores that can repeat the harm without meaning to 7. When a place treats your child like a person with a story, the rest of the work gets easier.
What keeps recovery going after the program ends
Peer recovery support and family involvement
The first weeks after a program ends are often the quietest and the riskiest. The structure falls away. The phone stops buzzing with appointment reminders. This is where two kinds of support tend to carry the most weight: people who have walked this road, and the family that’s still walking it alongside.
Peer recovery support specialists are people in their own sustained recovery, trained to come alongside your adult child as a coach, a confidant, and a practical helper. They show up for the awkward stuff — the first sober wedding, the urge that hits on a Sunday afternoon. The evidence review on peer services found reduced relapse rates, better treatment retention, stronger relationships with providers, and higher satisfaction with care overall 13.
Family involvement matters too, and not in a vague way. Family-based interventions are designed to help your child sustain recovery while also helping the rest of the household communicate, set limits, and tend to their own well-being 12. You are part of the recovery environment. Getting your own support isn’t a luxury — it’s part of what keeps the whole thing standing.
Telehealth as a bridge to continuing care
If you remember the version of treatment that meant driving across town three nights a week, the current version may surprise you. A lot of continuing care now happens by video. Therapy sessions, prescriber visits, group check-ins, and recovery coaching can all run through a laptop or a phone, which makes it easier for your adult child to stay connected when life gets busy or hard.
This shift isn’t a fringe experiment. SAMHSA’s tracking of treatment facilities showed the share offering telemedicine more than doubled in a single year, jumping from 27.5% in 2019 to 58.6% in 2020 15. What started as a pandemic workaround stayed because it worked.
A 2025 study looking at patients whose clinicians used a lot of telehealth versus a little found the high-telehealth group had more outpatient substance use visits and lower substance-use-related hospitalizations, without higher rates of overdose or relapse 14. Translation: people who could see their counselor from the kitchen table actually showed up more, and they were no worse off for it.
For your child, that might mean an early morning session before work, a quick check-in during lunch, or a Sunday group from the apartment couch. The barrier to staying in care drops, and so does the temptation to quietly drift away from it.
Harm reduction as a safety net, especially in Oregon
Harm reduction is often misunderstood as the opposite of treatment. It isn’t. It’s a set of practical tools designed to keep your adult child alive and as healthy as possible, whether they’re in active treatment, between programs, or somewhere in the long middle 8.
In Oregon, harm reduction shows up as naloxone distribution to reverse opioid overdoses, syringe service programs that prevent infections like HIV and hepatitis, and safer-use education that meets people where they are 8. Carrying naloxone in your purse doesn’t mean you’ve given up on recovery — it means you’ve accepted that recovery isn’t always a straight line, and a relapse doesn’t have to end in a funeral.
You can hold two things at once. You can hope for full, sustained recovery for your child, and you can also keep them breathing while they get there. Both are acts of love.
Putting it together: what a coherent path can look like
Imagine a Tuesday a few months from now. Your adult child started in medically supervised detox because the withdrawal risk was real and someone had to be watching at 3 a.m. After about a week, when their body had steadied and they could sit through a full conversation again, they stepped down into a partial hospitalization program — full days of group and individual therapy, evenings at home or in sober housing. A few weeks later, the schedule loosened into intensive outpatient three nights a week so they could go back to work without losing the structure.
Now they see a counselor weekly, meet with a prescriber every month for the medication that keeps cravings quiet, and join a peer recovery group from the kitchen table on Sunday nights. You’re in your own family sessions, learning what to say and what not to say. There’s naloxone in the drawer, just in case.

Check Your Coverage for Treatment Options Now
See if your insurance covers medically supervised detox and next-step recovery support.
Frequently Asked Questions
Is detox alone enough to help my adult child recover?
Detox handles the acute withdrawal window, but it doesn’t teach a person how to live without the substance. The strongest evidence points to medications plus behavioral therapy sustained over time as what produces lasting recovery 1. Think of detox as the doorway, not the room.
What is the difference between PHP and IOP?
Is medication-assisted treatment just trading one drug for another?
No. Methadone, buprenorphine, and naltrexone are FDA-approved medications that quiet cravings without producing the high of street opioids 18. A person on buprenorphine isn’t sedated — they show up to work and therapy clearer-headed. The evidence supports medication combined with counseling, not one alone 10.
How do clinicians decide which level of care my child needs?
Most use the ASAM six dimensions: withdrawal risk, other medical issues, mental health, readiness to change, relapse potential, and the safety of the home environment 3. Federal Medicaid guidelines lean on the same framework 2. Ask the intake clinician directly how they match a person to a level of care.
How long should treatment last to actually work?
NIDA finds that treatment lasting less than three months is often insufficient, and the best outcomes come with longer engagement across the continuum 1. That doesn’t mean three months in residential — it means three months or more of connected care, which might be a week of detox, several weeks of PHP, then months of IOP and outpatient.
What happens after a residential or detox program ends?
Continuing care is the part that holds. That usually means stepping down to PHP or IOP, weekly counseling, medication management if relevant, peer recovery support 13, and often family sessions 12. Telehealth makes many of these easier to keep up with 14. If you need referrals, SAMHSA’s free 24/7 helpline can point the way 9.
References
- Treatment | National Institute on Drug Abuse (NIDA). https://nida.nih.gov/research-topics/treatment
- Overview of Substance Use Disorder (SUD) Care Clinical Guidelines. https://www.medicaid.gov/state-resource-center/innovation-accelerator-program/iap-downloads/reducing-substance-use-disorders/asam-resource-guide.pdf
- The ASAM Criteria® At a Glance: The Six Dimensions of Multidimensional Assessment. https://www.azahcccs.gov/PlansProviders/Downloads/CurrentProviders/ASAMCriteriaBrochure.pdf
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Cognitive-Behavioral Therapy for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC2897895/
- Integrating Treatment for Co-Occurring Mental Health Conditions. https://pmc.ncbi.nlm.nih.gov/articles/PMC6799972/
- Trauma-Informed Approaches and Programs. https://www.samhsa.gov/mental-health/trauma-violence/trauma-informed-approaches-programs
- Oregon Health Authority: Harm Reduction. https://www.oregon.gov/oha/ph/preventionwellness/substanceuse/pages/harm-reduction.aspx
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- TIP 63: Medications for Opioid Use Disorder. https://www.samhsa.gov/resource/ebp/tip-63-medications-opioid-use-disorder
- Community-based psychosocial substance use disorder interventions in low- and middle-income countries. https://pmc.ncbi.nlm.nih.gov/articles/PMC7542947/
- Chapter 3—Family Counseling Approaches. https://www.ncbi.nlm.nih.gov/books/NBK571088/
- Peer Recovery Support for Individuals With Substance Use Disorders. https://www.mass.gov/doc/peer-research-review-submitted-by-kim-krawczyk/download
- The impact of increased telehealth use on the treatment of patients with substance use disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC11978320/
- Telemedicine Services in Substance Use and Mental Health Treatment Facilities. https://www.samhsa.gov/data/report/telemedicine-services
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Chapter 5—Specialized Substance Abuse Treatment Programs. https://www.ncbi.nlm.nih.gov/books/NBK64815/
- An Overview of Medication-Assisted Treatment for Opioid Use Disorders. https://icjia.illinois.gov/researchhub/articles/an-overview-of-medication-assisted-treatment-for-opioid-use-disorders-for-criminal-justice-and-substance-use-treatment-professionals
- Managing Life with Co-Occurring Disorders. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. https://www.pathwaysrtc.pdx.edu/focal-point-S1510
- Chapter 4. Outpatient and Intensive Outpatient Treatment for Substance Use Disorders. https://www.ncbi.nlm.nih.gov/books/NBK64094/
- Partial hospitalization and IOP | Ohio State Medical Center. https://wexnermedical.osu.edu/mental-behavioral/partial-hospitalization-iop


