Key Takeaways
- Rapid medical detox uses general anesthesia or deep sedation with opioid antagonists like naltrexone to compress opioid withdrawal into 4 to 8 hours 6.
- Peer-reviewed evidence has not shown that anesthesia-assisted detox improves long-term recovery over standard medically supervised withdrawal, and a 2012 CDC investigation found two deaths and five serious adverse events among 75 patients at one clinic 1, 7.
- Rapid detox was designed for opioids, not alcohol or benzodiazepines, and tolerance drops sharply afterward, making relapse in the following days or weeks a serious overdose risk 4.
- Detox is only the first step; lasting recovery depends on medication-assisted treatment with buprenorphine, methadone, or naltrexone, plus therapy and ongoing outpatient care 3, 8.
The Promise vs. the Reality of a ‘Fast’ Detox
If you’re reading this while you’re sick, shaky, or watching someone you love shake, take a breath. The fact that you’re looking for real answers is already a step that matters.
You’ve probably seen the pitch: go to sleep addicted and wake up clean, past withdrawal. This idea, often marketed as rapid medical detox, anesthesia-assisted rapid opioid detoxification (AAROD), or ultra-rapid opioid detox (UROD), involves using sedation or full anesthesia with opioid receptor blockers to shorten the withdrawal period 6. It is a real medical procedure, but the marketing often differs significantly from the scientific evidence.
Peer-reviewed evidence has not demonstrated that rapid detox leads to better long-term recovery compared to standard, medically supervised withdrawal 7. Moreover, it carries serious risks that regular detox does not, primarily because general anesthesia can be genuinely tricky for a body already stressed by dependence 6. No detox, fast or slow, addresses the underlying reasons for substance use.
What you truly want is quick access to care, rapid relief from severe symptoms, and a safe path through the initial 5 to 7 days. These are achievable goals that do not require anesthesia. This article will explain what rapid detox truly entails, outline safer alternatives, and help you distinguish between programs that genuinely help and those that are merely selling a quick fix.
What Rapid Medical Detox Actually Means
The term “rapid detox” is often used loosely, leading to confusion. It specifically refers to a procedure where you are placed under sedation or full general anesthesia. While unconscious, high doses of opioid antagonists, such as naltrexone or naloxone, are administered. These medications flood your brain’s opioid receptors, forcing your body to undergo withdrawal in a matter of hours rather than days 6. The goal is for the acute physical withdrawal to be largely complete by the time you regain consciousness.
It’s crucial to clarify what a program means by “rapid detox.” Some clinics refer to the anesthesia-based procedure, while others use the term more broadly to mean “fast, medically supervised withdrawal management with comfort medications,” which is a very different approach. When inquiring about programs, always ask directly if general anesthesia or deep sedation is involved, as this significantly alters the risk profile.
Rapid medical detox was initially developed for opioid dependence, including heroin, prescription painkillers, and fentanyl. It is not standard practice for alcohol or benzodiazepine withdrawal, as these substances involve different biological pathways and carry distinct, life-threatening risks that anesthesia does not resolve.
It’s important to understand that detox, regardless of its duration or method, only addresses the acute physical aspect of withdrawal. It clears the substance from your system and helps your body reset. It does not tackle cravings that may emerge later, nor does it help rebuild aspects of your life that have been affected. This is why major medical bodies consider detox as merely the first step in treatment, not the entire solution 8. Understanding this distinction is vital for asking the right questions and ensuring your safety.
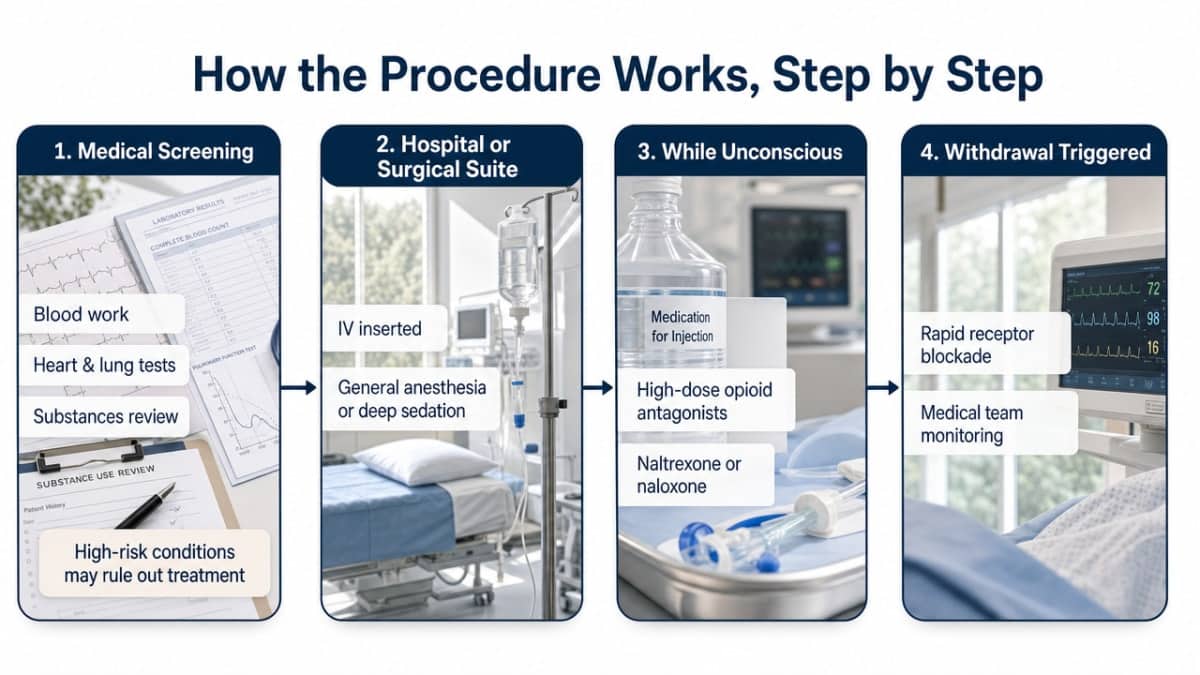
How the Procedure Works, Step by Step
Here’s a realistic overview of what happens during a rapid detox procedure, beyond the marketing descriptions.
- Pre-procedure screening. Before the procedure, you undergo medical screening, including blood work, heart and lung function tests, and a review of all substances in your system. Anesthesia is safer for a healthy body, but opioid dependence inherently stresses the body 6. Conditions like heart disease, breathing problems, hepatitis, or severe depression can increase risks. A responsible program will decline treatment if the risks outweigh the potential benefits.
- Anesthesia and antagonist administration. On the day of the procedure, you are taken to a hospital or surgical suite. An IV is inserted, and you receive general anesthesia or deep sedation, similar to what’s used for surgery. Once unconscious, the medical team administers high doses of opioid antagonists, typically naltrexone or naloxone. These medications bind to opioid receptors in your brain, displacing existing opioids and inducing rapid withdrawal 6.
- Monitored withdrawal under sedation. While you are under anesthesia, your body still experiences withdrawal symptoms, such as increased heart rate, blood pressure fluctuations, sweating, and cramping. You do not consciously feel these symptoms. The medical team monitors you closely and manages these physical reactions in real-time. The procedure itself usually lasts 4 to 8 hours.
- Recovery and discharge. After the anesthesia wears off, the peak of acute withdrawal is over, but you are not fully recovered. Most individuals wake up feeling exhausted, nauseated, achy, and with muscle pain that can persist for days or even weeks 9. This prolonged recovery period is often omitted from marketing materials. You are typically discharged the same day or the next, often with a naltrexone regimen to continue blocking opioid effects. The success of recovery then depends on subsequent steps, such as therapy, medication support, and a comprehensive recovery plan.
The Safety Question You Deserve a Straight Answer To
You deserve honest information about safety, not just reassurance. The available data provides a clear picture.
A notable safety report on rapid detox comes from a CDC investigation of an outpatient clinic in New York City. Between January and September 2012, out of 75 patients who underwent anesthesia-assisted rapid opioid detoxification, two died and five experienced serious adverse events requiring hospitalization 1. While this represents a single clinic’s experience, it prompted New York City health officials to recommend that providers avoid AAROD in favor of evidence-based options for opioid dependence treatment 2. This recommendation remains in effect.
The risks associated with rapid detox stem from several factors. General anesthesia is a significant medical intervention with inherent risks, even for healthy surgical patients. When applied to a body already compromised by opioid dependence, and then subjected to rapid, forced withdrawal, the cardiovascular and metabolic strain is substantial. This can lead to dangerous fluctuations in blood pressure, heart rhythm problems, and pulmonary edema (fluid in the lungs). Rare but severe complications, such as subarachnoid hemorrhage (bleeding around the brain), have also been documented in connection with anesthesia-assisted detox 10.
It’s important to distinguish that medically supervised withdrawal, utilizing comfort medications and continuous monitoring, has a strong safety record. The added risk in rapid detox comes from the anesthesia, and studies have not shown that this increased risk is offset by better long-term outcomes 7. If a program claims rapid detox is uniformly safe, their claims are not supported by evidence. It is essential to ask probing questions.
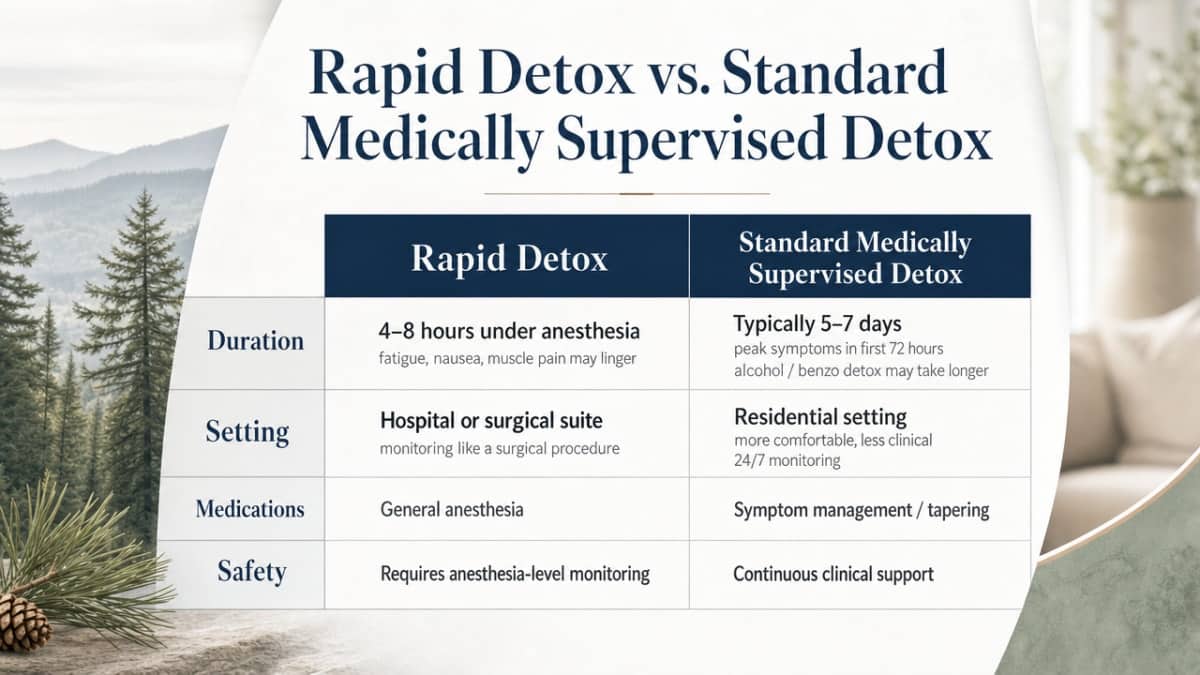
Rapid Detox vs. Standard Medically Supervised Detox
Comparing rapid detox and standard medically supervised detox reveals distinct differences, despite their shared goal of helping the body through withdrawal.
- Duration
- Rapid detox condenses acute withdrawal into approximately 4 to 8 hours under anesthesia, though lingering fatigue, nausea, and muscle pain can last for days or weeks 9. Standard medically supervised detox for opioids typically spans 5 to 7 days, with peak symptoms usually occurring within the first 72 hours 4. Alcohol or benzodiazepine detox may take longer due to careful tapering.
- Setting
- Rapid detox requires a hospital or surgical suite due to the use of general anesthesia, necessitating monitoring similar to any surgical procedure 6. Standard detox can occur in a residential setting that feels more comfortable and less clinical, offering 24/7 medical monitoring, a restful environment, and regular staff check-ins. Many find the calmer atmosphere more conducive to recovery.
- Medications
- Rapid detox relies on general anesthesia or deep sedation combined with high doses of opioid antagonists like naltrexone or naloxone to induce immediate withdrawal 6. Standard detox employs a different set of medications. For opioids, this includes buprenorphine, methadone, naltrexone (once stable), and lofexidine to alleviate acute symptoms 3. For alcohol and benzodiazepines, a careful taper of longer-acting benzodiazepines is used. The medications in standard detox have strong long-term evidence for supporting sustained recovery from opioid use 3.
- Safety Concerns
- Standard medically supervised detox has a well-established safety record when conducted with proper monitoring. In contrast, rapid detox does not. The 2012 CDC investigation in New York City reported 2 deaths and 5 serious adverse events among 75 patients 1. Furthermore, medical literature comparing anesthesia-assisted detox with buprenorphine- or clonidine-assisted detox has not shown that adding anesthesia improves long-term outcomes 7. This means rapid detox involves greater risk without a proven benefit.
When considering these options, rapid detox offers a shorter, riskier process without improving long-term recovery rates. Standard detox with comfort medications is a slower initial process but provides a more stable foundation for recovery. It also allows for therapy and follow-up care to begin during stabilization, rather than after discharge, which is crucial for lasting sobriety.
If You’re Withdrawing Right Now: Opioids, Alcohol, or Benzos
The substance you are withdrawing from significantly impacts the medical urgency and necessary approach. Read the section that applies to you, and if unsure, treat it as the more serious category and seek immediate help.
If it’s opioids (heroin, fentanyl, oxycodone, hydrocodone, methadone, or an unknown substance), withdrawal symptoms will be severe: deep aches, sweating, chills, cramps, vomiting, diarrhea, and restless legs. While intensely uncomfortable, opioid withdrawal is generally not life-threatening 4. The primary danger lies in the period after withdrawal. Your tolerance drops rapidly, making a previously routine dose potentially fatal if you relapse 4. This is why attempting to detox alone at home is extremely risky and often leads to overdose. Medically supervised detox with comfort medications like buprenorphine or lofexidine can alleviate severe symptoms and, critically, transition you directly into ongoing care 3.
If it’s alcohol, withdrawal can be life-threatening. Initial symptoms like shaking, sweating, and anxiety within the first 24 hours can escalate to seizures or delirium tremens (DTs), a medical emergency characterized by confusion, rapid heart rate, and dangerous blood pressure fluctuations. If you have been drinking heavily daily, especially for years, do not stop abruptly at home. Seek immediate care at a detox facility or emergency room. Standard medically supervised detox uses a carefully managed benzodiazepine taper and continuous monitoring to ensure your safety during this critical period.
If it’s benzodiazepines (Xanax, Klonopin, Ativan, Valium), the same severe warning applies, with even less room for error. Benzodiazepine withdrawal can trigger seizures and severe autonomic instability, and these symptoms can appear days after your last dose, not just hours. Never attempt to quit these medications on your own. A slow, medically managed taper is the only safe approach, and it typically takes longer than opioid or alcohol detox.
None of these situations call for general anesthesia. Rapid detox was designed for opioids, and even for them, evidence does not show it surpasses standard care 7. What you need in the next 24 hours is a call to a detox program or a hospital, not a procedure that puts you under.
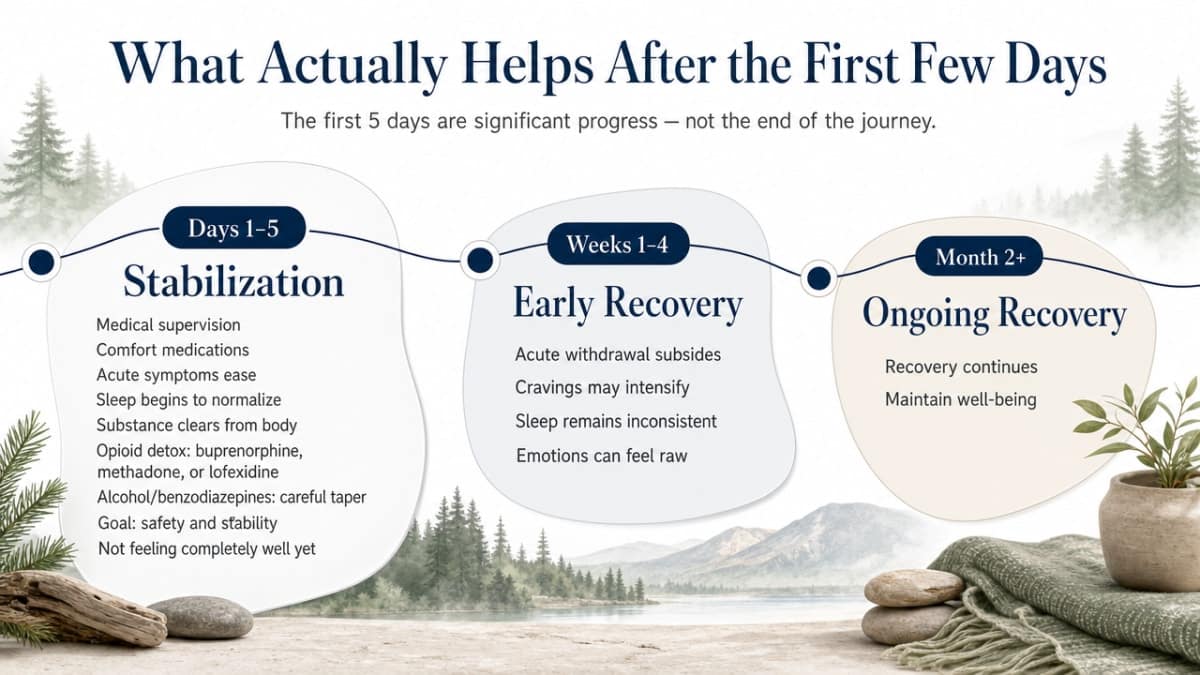
What Actually Helps After the First Few Days
Getting through the initial 5 days of detox is significant progress, but it’s not the end of the journey. It’s the beginning of the work required to maintain well-being.
Consider recovery in three distinct phases:
Days 1 through 5: Stabilization. This is the medically supervised phase where comfort medications ease acute symptoms, sleep patterns begin to normalize, and the substance clears from your body. For opioid detox, medications like buprenorphine, methadone, or lofexidine are crucial for symptom management 3. For alcohol or benzodiazepines, a careful taper prevents seizures. The goal here is safety and stability, not feeling completely well.
Weeks 1 through 4: Early Recovery. This period can be challenging. Acute physical withdrawal subsides, but cravings often intensify, sleep remains inconsistent, and emotions can feel raw. This is where medication-assisted treatment (MAT) becomes vital. Buprenorphine, methadone, and naltrexone are FDA-approved medications for opioid use disorder, with strong evidence supporting their long-term benefits 3. These medications stabilize brain chemistry altered by dependence. Alongside MAT, therapy—individual, group, or family sessions—helps build routines for sustained recovery.
Month 2 and beyond: Ongoing Care. This phase significantly improves long-term outcomes. Detox alone, without follow-up care, has poor long-term success rates, which is why clinical guidelines consider detox as one step within a broader treatment plan 8. Ongoing outpatient care, such as partial hospitalization, intensive outpatient programs, or regular therapy, ensures medication adherence, provides support during difficult times, and connects you with a community of peers. Opioid use disorder is recognized as a chronic, treatable condition 3, meaning it requires ongoing management but allows for a fulfilling life.
If a program presents detox as a standalone solution, it’s essential to ask about their plan for day 6 and beyond. Trustworthy programs will have a comprehensive strategy for continued care.
How to Choose a Detox Program Without Getting Sold To
When you or a loved one is in distress, a reassuring voice on the phone can seem like the perfect solution. However, it’s crucial to discern genuine help from a sales pitch. Here’s how to evaluate programs:
Ask about the plan for day 6. A program that focuses solely on getting you “clean” without detailing subsequent steps is likely marketing detox as a final solution. Federal guidelines emphasize that withdrawal management is just one component of a longer treatment plan 8. You should expect a clear answer that includes therapy sessions, a partial hospitalization or intensive outpatient track, continued medication support post-discharge, and family involvement if desired.
Inquire about the specific medications used. For opioid withdrawal, evidence-based options include buprenorphine, methadone, naltrexone (once stable), and lofexidine for acute symptoms 3. For alcohol or benzodiazepine withdrawal, the term “taper” should be mentioned. Be wary of programs that prioritize general anesthesia and high-dose antagonists, as this indicates the anesthesia-assisted procedure that New York City health officials have advised against in favor of evidence-based alternatives 2.
Clarify the setting. There’s a significant difference between a home-like residential space with 24/7 medical monitoring, a surgical suite, or a bed in a hallway. You have the right to know the environment you will be entering.
Ask what happens if a relapse occurs. Reputable programs will have a clear answer, acknowledging that opioid use disorder is a chronic, treatable condition 3. Programs that become uncomfortable with this question may be less focused on long-term recovery.
Remember, you are always allowed to end a call. If a program pressures you to make an immediate decision, that pressure serves their interests, not yours. Any reputable option, like Pacific Crest Trail Detox, will still be available after you take time to breathe and ask thorough questions.
Check Your Coverage for Rapid Medical Detox
Find out if your insurance supports safe, medically supervised detox right now.
Frequently Asked Questions
Is rapid medical detox safe?
Rapid medical detox carries significant risks that standard medically supervised detox does not. General anesthesia, when administered to a body already stressed by opioid dependence, can lead to severe cardiovascular and metabolic complications. Following a review of patient outcomes, New York City health officials recommended avoiding anesthesia-assisted rapid opioid detoxification in favor of evidence-based options 2. Standard detox, which uses comfort medications and 24/7 monitoring, has a much stronger safety record and is supported by more robust long-term evidence 3.
How long does rapid medical detox take compared to standard detox?
The rapid detox procedure itself lasts approximately 4 to 8 hours under anesthesia, but many individuals experience lingering fatigue, nausea, and muscle pain for days or weeks afterward 9. Standard medically supervised opioid detox typically takes 5 to 7 days, with the most intense symptoms peaking within the first 72 hours 4. Detox for alcohol and benzodiazepines often requires a longer duration due to the need for careful tapering. While rapid detox offers a shorter acute phase, this does not translate to improved long-term recovery outcomes 7.
Can I die from alcohol or benzodiazepine withdrawal at home?
Yes, withdrawal from heavy alcohol use can progress to seizures and delirium tremens, which involve dangerous fluctuations in heart rate and blood pressure. Similarly, benzodiazepine withdrawal (from drugs like Xanax, Klonopin, or Ativan) can trigger seizures and severe autonomic instability, sometimes days after the last dose. It is critical not to stop these substances abruptly at home. Seek immediate medical attention at a detox facility or emergency room, where a medically supervised taper can ensure your safety.
Will I still feel withdrawal symptoms if I’m sedated during rapid detox?
While you won’t consciously feel the acute peak of withdrawal because you are unconscious, your body still undergoes withdrawal processes, including elevated heart rate, blood pressure swings, sweating, and cramping 6. After the anesthesia wears off, most people wake up feeling exhausted, nauseated, and achy, with muscle pain and disrupted sleep that can persist for days or weeks 9. The procedure compresses the most intense hours but does not eliminate withdrawal, and the aftermath is often more challenging than marketing suggests.
What happens after detox ends?
Detoxification clears the substance from your body but does not address cravings, sleep disturbances, or emotional challenges that often emerge in the weeks following. Federal guidance considers withdrawal management as just one step within a comprehensive treatment plan 8. Effective long-term recovery relies on ongoing care, including medication-assisted treatments like buprenorphine, methadone, or naltrexone for opioid use disorder, combined with therapy and regular outpatient support 3. Additionally, your tolerance drops significantly after detox, making relapse without a plan a serious overdose risk 4. It is crucial to establish the next steps for ongoing care before completing detox.
How do I know if a detox program is legitimate?
A legitimate program will have a clear answer for what happens on day 6, detailing therapy, medication support, and outpatient follow-up, as detox alone is not a long-term solution 8. Inquire about the specific medications they use; for opioids, you should hear buprenorphine, methadone, naltrexone, or lofexidine 3, and for alcohol or benzodiazepines, the term “taper” is essential. Be cautious of any program that emphasizes general anesthesia or pressures you to make a quick decision. Reputable programs will allow you time to consider your options.
References
- Deaths and Severe Adverse Events Associated with Anesthesia-Assisted Rapid Opioid Detoxification — New York City, 2012. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6238a1.htm
- Deaths and severe adverse events associated with anesthesia-assisted rapid opioid detoxification–New York City, 2012. https://pubmed.ncbi.nlm.nih.gov/24067581/
- Medications for Opioid Use Disorder | National Institute on Drug Abuse. https://nida.nih.gov/research-topics/medications-opioid-use-disorder
- Opiate and opioid withdrawal: MedlinePlus Medical Encyclopedia. https://medlineplus.gov/ency/article/000949.htm
- Pharmacological strategies for detoxification – PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4014033/
- Ultrarapid opiate detoxification: a review. https://pubmed.ncbi.nlm.nih.gov/12944440/
- Anesthesia-Assisted vs Buprenorphine- or Clonidine-Assisted Heroin Detoxification and Naltrexone Induction. https://pubmed.ncbi.nlm.nih.gov/201451/
- Detoxification and Substance Abuse Treatment – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK64115/
- Main Study Findings and Author’s Conclusions. https://www.ncbi.nlm.nih.gov/books/NBK343896/
- Managing Subarachnoid Hemorrhage Precipitated by Anesthesia …. https://pmc.ncbi.nlm.nih.gov/articles/PMC8885228/