Key Takeaways
- Alcohol withdrawal can escalate into seizures and delirium tremens, and cold-turkey attempts at home miss the monitoring and benzodiazepine dosing that prevent deaths.4,9
- Opioid detox feels survivable but sharply lowers tolerance, so unsupervised attempts raise overdose risk — buprenorphine or methadone cut mortality where willpower alone does not.6,10
- Benzodiazepine withdrawal can trigger seizures, and improvising with leftover pills is unsafe; a structured, medically supervised taper with measured doses is the correction.3,8
- Shortcuts like anesthesia-assisted rapid detox, kratom, and someone else’s pills carry real harm without reducing withdrawal — one CDC-reviewed clinic saw two deaths among 75 patients.14
- Treating detox as the finish line is why attempts collapse; ongoing medications, counseling, and structured follow-up are what keep the next relapse from becoming fatal.3,8
The 3 A.M. Shakes and Why This Keeps Happening
It’s 3:17 a.m. You’ve been counting hours since your last drink — or your last pill — the way other people count sheep. Your hands won’t stop trembling. The sheets are damp. Your heart is doing something your heart shouldn’t do, and the only thought louder than the nausea is: not again.
If you’ve tried to detox at home before and it didn’t stick, please hear this first: you are not weak. You are not failing at willpower. You are trying to talk your body out of a medical event, and bodies don’t negotiate.
Withdrawal from alcohol, benzodiazepines, and opioids isn’t a bad mood you can outlast in a locked bathroom. It’s a physical process with real vital signs attached — blood pressure, heart rate, seizure risk, and for some people, delirium that can turn dangerous fast. The medical guidelines that treatment programs follow describe withdrawal as a condition that requires assessment, monitoring, and often medication — not a test of grit.4,9
That’s the piece most people miss when they try to do this alone. You didn’t want to be a burden. You didn’t want anyone to know. You wanted to handle it quietly before Monday, perhaps thinking a non medical detox approach would suffice. And every time the shaking got bad enough, you reached for the thing that made it stop — because the thing that made it stop was working exactly the way your nervous system had learned to expect.
That isn’t a moral failure. That’s chemistry.
What follows isn’t a lecture. It’s a plain-language walk through why non-medical detox keeps ending the same way, what actually makes it safer, and what a believable next step can look like — even at 3 a.m., even after several tries.
What ‘Non-Medical Detox’ Actually Means
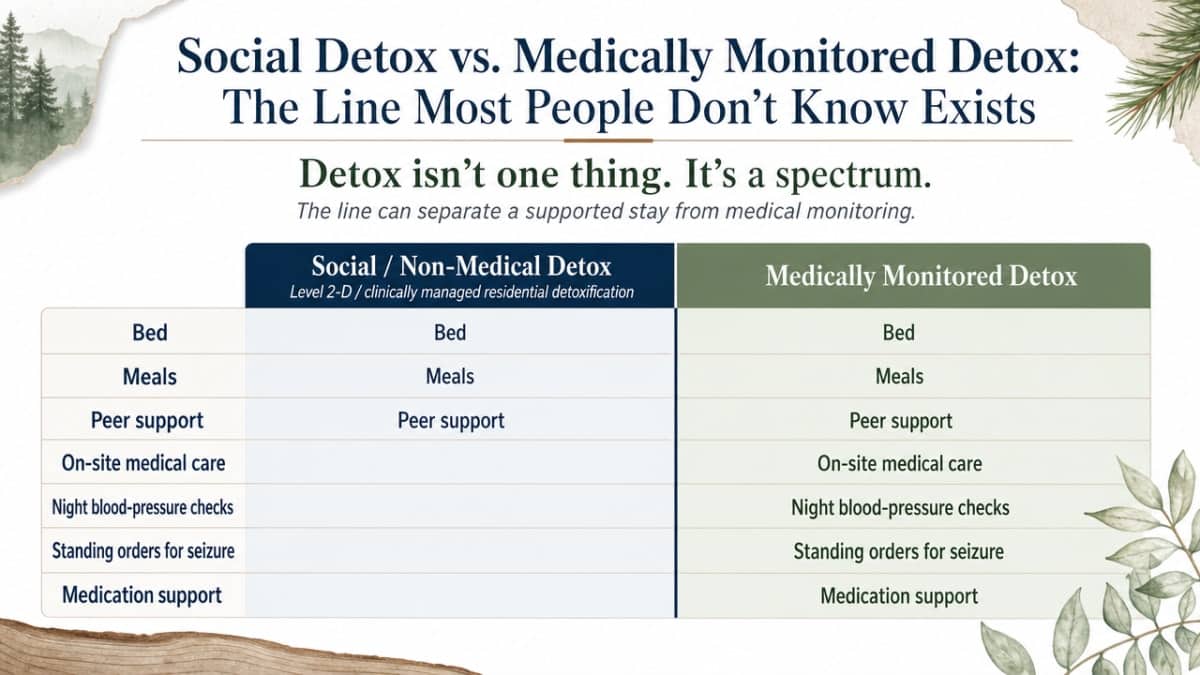
Social Detox vs. Medically Monitored Detox: The Line Most People Don’t Know Exists
Here’s something almost no one explains before you’re already in it: “detox” isn’t one thing. It’s a spectrum, and the difference between the levels can be the difference between a safe week and a 911 call.
When you call a program, the language they use tells you which end you’re on. SAMHSA’s clinician guide describes what’s called Level 2-D — clinically managed residential detoxification, sometimes just called “social detox”. It offers a bed, meals, and peer support. What it doesn’t offer is on-site medical care. No nurse checking your blood pressure at 2 a.m. No standing orders for a seizure. No medication to soften what your nervous system is about to do.13
The CSAT chapter on levels of care puts it plainly: social detox programs provide “room, board, and interpersonal support” but not medical treatment. For a lot of people, that’s genuinely not enough — especially if the substance is alcohol, benzodiazepines, or a mix.1
Medically monitored detox is a different level of care. It means 24-hour nursing, a physician overseeing your case, medications available for withdrawal symptoms, and a real plan if things escalate. It doesn’t have to look like a hospital. It can be a house with regular bedrooms and a kitchen — the medical part is who’s staffing it and what’s on the shelf, not the paint on the walls.1,13
Two words that sound alike — one important difference
| Social / Non-Medical Detox (Level 2-D) | Medically Monitored Detox |
|---|---|
| Room, board, peer support | Room, board, peer support |
| No on-site medical services | 24-hour nursing and physician oversight |
| No withdrawal medications on-site | Medications available to ease withdrawal |
| No seizure or DT protocol | Seizure and delirium protocols in place |
When you call a program, you can ask directly: Is there a nurse on-site 24 hours a day? Do you have medications available for withdrawal? What’s your protocol if I have a seizure? The answers tell you which level you’re actually calling.
The Home Attempts People Actually Try
Non-medical detox isn’t just what happens inside a facility with the wrong staffing. Most of the time, it’s what happens on a couch.
You’ve probably tried some version of this already. It usually looks like one of a few patterns, and none of them make you foolish — they make you someone who was trying to solve a hard problem with what you had.
- Cold turkey behind a closed door. Pouring out the bottle on Sunday night. Deleting the contact. Powering through Monday. It works for a headache, so it feels like it should work here.
- Tapering with whatever’s in the drawer. Cutting your Xanax in half. Stretching an old prescription across a week. Trying to “come down slowly” using pills that weren’t dosed for tapering and weren’t measured with anyone’s help.
- The one-drink-less method. Two beers instead of six. Then two the next night, then two the next, waiting for the count to fall on its own. Except by day three the shakes tell you the math isn’t working.
- Kratom, CBD, sleep aids, whatever’s on the shelf at the gas station. Trying to blunt the worst of it with something that isn’t the drug.
- A friend’s spare bedroom. Someone kind offering to “sit with you.” Real love. No blood pressure cuff.
All of these are, technically, non-medical detox. The reason they keep collapsing isn’t that you didn’t try hard enough. It’s that none of them include the two things withdrawal from alcohol, benzos, or opioids actually needs: someone watching your vitals, and the right medication when your body asks for it. Recognizing which of these you’ve been doing isn’t defeat. It’s the first honest data point.9,8
Alcohol: Why Cold Turkey Can Kill You
You’ve probably heard people quit drinking cold turkey and be fine. That’s true. It’s also survivor bias — the ones who weren’t fine aren’t the ones telling the story at brunch.
Alcohol is the substance that quietly kills the most people during unsupervised withdrawal, and the reason is chemistry, not character. When you’ve been drinking heavily for a long time, your brain adapts by turning down its natural calming signals and turning up the excitatory ones. Take the alcohol away suddenly, and the calming brake is gone — but the accelerator is still floored. That’s when the shakes, the racing heart, the sweats, and in some cases seizures and delirium tremens show up.4
Delirium tremens isn’t a rough night. It’s confusion, hallucinations, fever, blood pressure spikes, and a mortality rate that turns a bathroom floor into an emergency room. The medical literature is consistent that severe alcohol withdrawal is a medical event that needs assessment, monitoring, and medication — usually benzodiazepines dosed carefully by clinicians — to prevent seizures and death.4,9
Here’s the part that trips a lot of people up: you can’t reliably predict who will have severe withdrawal from how much you drank last week. History matters. Prior withdrawal episodes, other health conditions, how long you’ve been drinking daily — these shift the risk in ways a person shaking alone on a couch can’t score themselves for.9
If you tried before and “powered through,” that doesn’t mean the next time will be the same. Withdrawal can get worse with each attempt — a pattern clinicians call kindling — which is why what worked (barely) at 32 can put someone in the ICU at 41.4
Opioids: Why ‘Just Getting Through It’ Backfires
Opioid withdrawal has a reputation problem. People will tell you it feels awful but won’t kill you — flu-like, sweaty, sleepless, humbling, but survivable. That’s mostly true in the moment. It’s also the reason opioid detox is one of the most dangerous things to do alone, because the risk isn’t during the worst days. The risk is what comes after.
Here’s the piece that keeps catching people who thought they were finally through the hard part. Your tolerance drops fast during withdrawal. The dose that used to just get you level a week ago can stop your breathing today. If you white-knuckle through five days, feel proud, then relapse the way most people do at some point — the amount your body used to handle isn’t the amount your body can handle anymore.
That’s not a moral story about slipping. It’s a pharmacology story about a smaller person on the same dose.
A large real-world study of people with opioid use disorder found that short-term detox and long-term rehab without medications were no more effective than no treatment at all for preventing overdose death, while buprenorphine and methadone significantly cut mortality. Read that twice. Trying hard, alone, without medication, was not better than doing nothing — because doing nothing at least didn’t lower the tolerance that later turned an ordinary dose into an overdose.6
The medications that change this outcome aren’t punishment and they aren’t substituting one drug for another in the way the internet argues about. Buprenorphine and methadone occupy the same receptors that heroin, fentanyl, oxycodone, and hydrocodone act on — but steadily, without the rollercoaster — so your brain isn’t screaming and your risk of dying drops 10, 5. Major clinical guidelines recommend offering one of these as first-line care for opioid detox, not as a last resort.12,3
None of this means what you’ve been through doesn’t count. Every day you’ve stayed alive counts. It just means the version of “trying harder” that leaves out medication is the version that keeps costing people their lives — and it doesn’t have to keep being your version.
Benzodiazepines: The Taper You Can’t Improvise
If alcohol is the one that surprises people and opioids are the one people underestimate, benzodiazepines are the one that punishes improvisation. Xanax, Klonopin, Ativan, Valium — the pills that were supposed to help you sleep, or take the panic down a notch, or get through a hard year. And then, somewhere along the way, the pills became the thing you couldn’t stop taking without your body coming apart.
Trying to quit benzos on your own makes complete sense. You probably started with a legitimate prescription. Asking for help feels like admitting something you weren’t ready to name. So you started cutting pills in half, or stretching what was left, or just stopping when the bottle ran out.
Here’s the truth that isn’t a scolding: benzodiazepine withdrawal can trigger seizures, and the taper needed to prevent that isn’t something you can eyeball with what’s left in the drawer. WHO-linked guidelines describe benzodiazepine withdrawal as a condition that requires a structured, gradually reduced dose under medical supervision — not a guess. The same medication class that treats severe alcohol withdrawal is the class your body is now dependent on, which is exactly why abrupt stops are dangerous.3,4
A medically supervised taper uses measured doses, sometimes converts you to a longer-acting benzo for a smoother descent, and adjusts based on how you’re actually doing that day. That last part matters. Your nervous system isn’t a spreadsheet.8
If you’ve been cutting pills alone, you’re not in trouble. You’re in the exact place where a real taper — done with someone watching — is the honest next step.
Shortcuts That Hurt: Rapid Detox, Kratom, and Leftover Pills
When you’ve been shaking for a week and the internet is open at 2 a.m., shortcuts look like mercy. A one-day procedure that promises to skip the worst part. A powder that’s legal at the smoke shop. A friend’s spare Xanax. You’re not naive for looking. You’re tired.
The problem is that the shortcuts marketed hardest tend to carry the risks explained least.
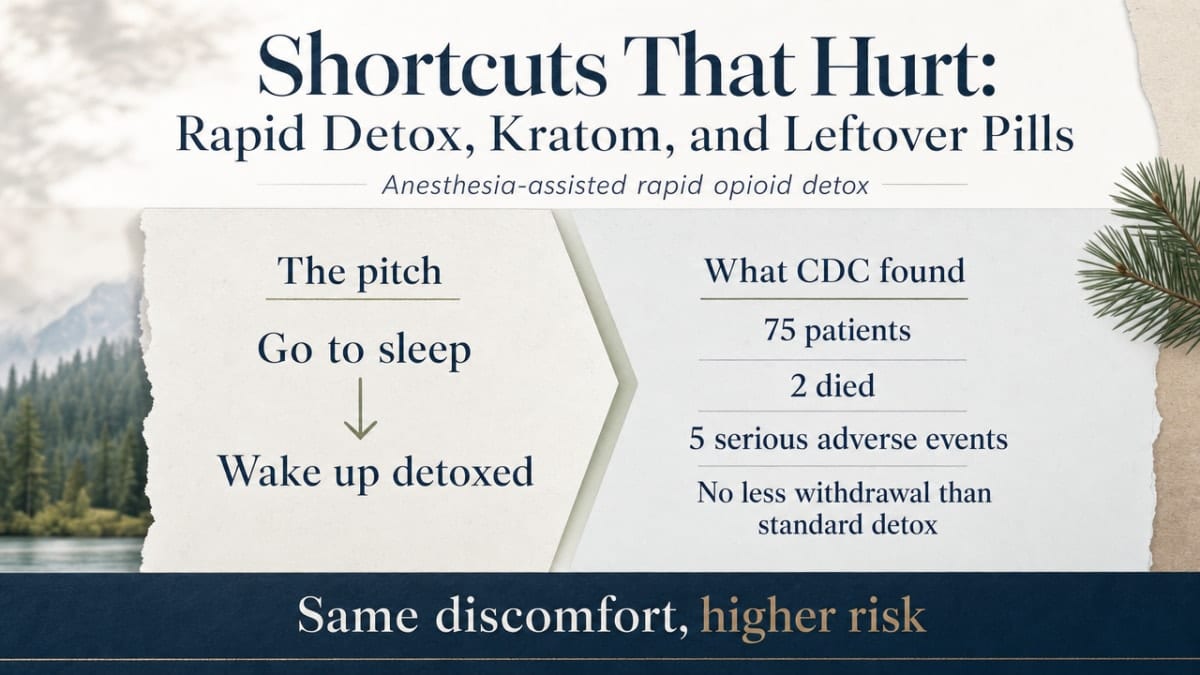
Anesthesia-assisted rapid detox. The pitch is powerful: go to sleep, wake up detoxed, skip the days on the bathroom floor. The evidence is harder to look at. A CDC investigation of a single New York City clinic in 2012 found that among 75 patients who underwent anesthesia-assisted rapid opioid detoxification, two died and five others had serious adverse events — and the procedure did not reduce withdrawal symptoms any more than standard detox. Same discomfort, higher risk of dying on the table.14
Anesthesia-assisted rapid opioid detox, single NYC clinic (2012):
2 deaths and 5 serious adverse events among 75 patients — with no reduction in withdrawal symptoms compared to standard detox.
Source: CDC MMWR, 2013.14
Kratom, and whatever the gas station is selling this month. Kratom acts on some of the same receptors as opioids, which is why it can dull withdrawal for a stretch and why people trade one dependence for another without meaning to. It isn’t dosed for tapering. It isn’t monitored. And when it stops working, you’re back where you started, plus a new withdrawal.
Someone else’s leftover pills. A partner’s old Klonopin. A parent’s Ativan from a rough year. The dose isn’t matched to what your body has adapted to, the taper isn’t measured, and if you have a seizure at 4 a.m. no one on the label is coming.
None of these are moral failures on your part. They’re what people reach for when the real thing feels out of reach. The through-line is the same: they promise to skip the medical part of a medical event, and that’s precisely the part that keeps you alive. If you’ve tried one of these already, that’s useful information, not shame — it tells you what to rule out next time you ask for help.5,8
What Safer Actually Looks Like
24/7 Medical Supervision and the Right Medications
Safer isn’t a mood or a mindset. It’s a room where someone is awake when you’re not, and a shelf with the right medication when your body finally asks for it.
In medically monitored detox, the basics are boring on purpose. A nurse takes your vitals on a schedule. A physician oversees your case and can adjust orders if something changes at 2 a.m. Medications are on-site — benzodiazepines dosed carefully for alcohol withdrawal to prevent seizures and delirium tremens, buprenorphine or methadone for opioid withdrawal so your brain isn’t screaming and your overdose risk drops, and a real, measured taper for benzodiazepines instead of a guess with what was left in the drawer.4,9,3,8,10,5
None of this requires a hospital ward with fluorescent lights and a shared bathroom. A residential medical detox can look like a house — bedrooms, a kitchen, a couch that’s actually comfortable — with the medical piece defined by who’s staffing it and what’s stocked, not by the paint on the walls. 1,11
The other quiet thing supervision buys you is honest assessment. A clinician can tell whether your withdrawal is trending mild, moderate, or dangerous, and adjust before you find out the hard way. The scoring tools exist because “how bad is this?” is not a question you can reliably answer about yourself while you’re shaking.9
What safer looks like, in one sentence: people watching your vitals, medicine that takes the edge off, and a room where nothing catastrophic gets to happen quietly. That’s the difference between white-knuckling and being cared for.
What Happens After Detox — the Part That Prevents the Next Attempt
Here’s the piece almost every failed attempt has in common: it treated detox like the finish line.
What comes after is where the next attempt gets prevented. For opioids, that often means staying on buprenorphine or methadone for as long as it helps — not as a weakness, as the treatment that keeps people alive. For alcohol and benzos, it means ongoing counseling, medications when appropriate, and a plan for the first hard Tuesday back home.10,6
The shape of “after” can look different depending on your life. Partial hospitalization for the first few weeks. Intensive outpatient sessions a few days a week. Standard outpatient counseling. Group therapy where you’re not the only one who tried this alone six times. Family sessions when the people who love you need help too.12
If previous attempts collapsed on day nine or day thirty, that’s not a verdict on you. It’s usually a sign that the after-part was missing. Building it in from the start — before you’re back in your kitchen wondering what to do next — is what turns “one more try” into the one that holds.
One Call, One Next Step
You don’t have to have this figured out tonight. You just have to make it smaller than it feels right now.
If you’re shaking, if you’re counting hours, if you’re staring at what’s left in the bottle or the pill container and doing the math again — the next step isn’t a plan for the next year. It’s a phone call.
Two numbers can start it. SAMHSA’s National Helpline is free, confidential, and open 24 hours a day, every day of the year, and it connects people to local treatment and detox referrals whether or not you have insurance. Calling doesn’t commit you to anything. It just puts a person on the other end of the line who has done this conversation before.7
The other kind of call is directly to a medically supervised detox program in your area. In the Portland and Milwaukie area, Pacific Crest Trail Detox provides that kind of 24/7 medically monitored detox in a home-like residential setting — with nursing, physician oversight, medications to ease withdrawal, and the after-part built in from day one. Ask any program you call the same three questions: Is there a nurse on-site around the clock? Do you have withdrawal medications available? What happens after detox?
You’ve already done the hardest part — you noticed the pattern, and you read this far. That counts. One more small step from here is enough for tonight.
Check Your Coverage for Medically Safe Detox
Find out if your insurance covers safer, medically supervised detox options today.
Frequently Asked Questions
Can I die from quitting alcohol cold turkey at home?
Yes, it’s possible — and that isn’t meant to scare you, it’s meant to be honest with you. Severe alcohol withdrawal can bring seizures and delirium tremens, both of which are medical emergencies. You can’t reliably predict your own risk from a couch. If you’ve been drinking heavily and daily, the safest move is a call, not a countdown.4,9
How is medically monitored detox different from social detox?
Social detox — sometimes called clinically managed residential detox — gives you a bed, meals, and peer support, but no on-site medical care. Medically monitored detox adds 24-hour nursing, a physician overseeing your case, and medications available when withdrawal hits. Same idea of a supportive place to land. Very different answer to the question, who’s here if my body starts doing something scary at 3 a.m.?1,13
Is it safe to taper off benzodiazepines using leftover pills?
Improvising a benzo taper with what’s left in the drawer isn’t safe, and it isn’t a fair fight either. Abrupt drops or uneven dosing can trigger seizures, and the right taper is a measured, gradually reduced dose under medical supervision — sometimes swapping to a longer-acting benzo for a smoother descent. If you’ve been cutting pills alone, that’s a sign to ask for a real taper, not more willpower.3,8
Why does opioid withdrawal feel survivable but still be dangerous?
The worst days feel awful but usually aren’t what kills people. The danger comes after. Your tolerance drops fast during withdrawal, so the dose your body used to handle can stop your breathing later. A large real-world study of people with opioid use disorder found detox and rehab without medications were no better than no treatment at preventing overdose death, while buprenorphine and methadone cut mortality.6
What about kratom or rapid detox under anesthesia — do those work?
Kratom acts on opioid receptors, so it can mask withdrawal for a stretch and quietly become its own dependence — no dosing plan, no monitoring. Anesthesia-assisted rapid detox has been linked to serious harm without any real advantage over standard detox in reducing withdrawal symptoms. Both promise to skip the medical part of a medical event, which is the part that keeps you safe.5,14
What happens if I’ve already failed detox several times?
It usually means the after-part was missing, not that you were. Detox is a transition, not a finish line, and withdrawal alone rarely produces lasting recovery — which is why medications and follow-up care matter as much as the first shaky week. Prior attempts are useful information for a clinician planning the next one. You’re not starting over. You’re starting with more data.3,8
References
- 2 Settings, Levels of Care, and Patient Placement (Treatment Improvement Protocol Series). https://www.ncbi.nlm.nih.gov/books/NBK64109/
- An Overview of Outpatient and Inpatient Detoxification. https://pmc.ncbi.nlm.nih.gov/articles/PMC6761814/
- Clinical Guidelines for Withdrawal Management and Treatment of Drug Dependence in Closed Settings. https://www.ncbi.nlm.nih.gov/books/NBK310652/
- Alcohol Withdrawal in Hospitalized Patients. https://www.ncbi.nlm.nih.gov/books/NBK604324/
- Main Study Findings and Author’s Conclusions (Detoxification and Substitution Treatments Review). https://www.ncbi.nlm.nih.gov/books/NBK343896/
- Treating opioid disorder without meds more harmful than no treatment at all. https://news.yale.edu/2023/12/19/treating-opioid-disorder-without-meds-more-harmful-no-treatment-all
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Pharmacological strategies for detoxification. https://pmc.ncbi.nlm.nih.gov/articles/PMC4014033/
- The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. https://pubmed.ncbi.nlm.nih.gov/32511109/
- Treatment Options for Substance Use Disorder. https://www.samhsa.gov/substance-use/treatment/options
- SETTINGS FOR OPIOID DETOXIFICATION. https://www.ncbi.nlm.nih.gov/books/NBK50626/
- Psychosocial interventions and opioid detoxification for drug misuse. https://pmc.ncbi.nlm.nih.gov/articles/PMC1934496/
- Quick Guide for Clinicians Based on TIP 45—Detoxification and Substance Abuse Treatment. https://nida.nih.gov/sites/default/files/samhsa_detoxification_and_substance_abuse_treatment.pdf
- Deaths and Severe Adverse Events Associated with Anesthesia-Assisted Rapid Opioid Detoxification — New York City, 2012. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6238a1.htm