
Key Takeaways
- Sustained recovery runs on stacked daily habits—sleep, connection, coping practice, movement, stable housing, and ongoing care—not willpower, since roughly 85% relapse within the first year.2
- Sleep quality is the foundation habit because poor sleep sharpens cravings, and a steady bedtime, phone across the room, and honest reporting to your care team break that loop.7
- Your environment and people shape the odds: recovery-supportive contacts, peer mentors, and sober housing roughly doubled two-year abstinence in one review compared with usual care.4,9,10
- Focus next on staying tied to care when you feel fine—keep medication, therapy, and meetings steady, and treat early drift signs like skipped sessions or bad sleep as the moment to reach out.1,3
What Early Recovery Actually Looks Like on a Tuesday
Tuesday morning, 6:47 a.m. You wake up before the alarm because your body still isn’t sure what to do with rest yet. The window is gray. Coffee helps, but not the way it used to. You check your phone. There’s a text from someone in your group that just says, “How’d you sleep?” You answer honestly for once. Bad. That small exchange is not a footnote to recovery. That is recovery.
Early recovery is quieter and stranger than most people expect. It’s not a montage. It’s a lot of ordinary hours to fill, and a nervous system that keeps asking, “Now what?” One study of adults in early substance use disorder recovery found that around 85% relapse within the first year. That number is not a verdict on you. It’s a description of how steep this stretch of the trail is, and why the people who make it through the year almost never do it on willpower alone. They rely on habits that sustain recovery—small, repeatable habits that stack up: sleep, connection, coping practice, movement, staying tied to care.2
This piece walks through those habits one by one, with real Tuesday-shaped examples. If you just finished medical detox at Pacific Crest Trail Detox or somewhere like it, or you’re helping someone who did, think of this as the map for the miles that come after the hardest part is technically over.

Sleep First: The Habit That Makes Every Other Habit Possible
If you only pick one habit to fight for in the first ninety days, make it sleep. Not because it’s easy — early recovery sleep is often broken, shallow, or absent entirely — but because everything else you’re trying to do gets harder without it. Cravings sharpen. Mood dips. The small annoyance of a slow line at the grocery store becomes the reason you’re gripping your car keys in the parking lot, deciding.
Researchers at Penn State studying people in opioid recovery found a direct link: patients who reported lower sleep quality also reported higher-than-usual drug cravings. That’s the loop you’re trying to break. Bad night, louder cravings, harder day, worse night. It compounds fast.7
Here’s what a sleep habit actually looks like on an ordinary weeknight in Milwaukie or Portland. Same bedtime, give or take twenty minutes. Phone on the far side of the room by 10 p.m. No screens once you’re in bed — not because a rule says so, but because your nervous system is still recalibrating and it needs the darkness. A short wind-down: a shower, a few pages of something boring, lights low. If your mind won’t quiet, write down what it’s chewing on. One sentence. Close the notebook.
Some of this will feel silly. Do it anyway. If you’re taking medication that steadies cravings — the kind of medication support Pacific Crest Trail Detox helps set up during and after detox — take it at the same time each night so your body learns the rhythm. If you’re waking at 3 a.m. drenched and anxious, tell your care team. Post-acute withdrawal messes with sleep for weeks, sometimes months, and there are things that help. You don’t have to white-knuckle through it alone. A rough night isn’t a failure. It’s information, and it’s the first place to bring in support.
The People Around You Are a Habit, Too
Shifting the Mix: Recovery-Supportive vs. Still-Using Contacts
Nobody wants to hear that recovery might mean fewer texts from certain people. It’s one of the harder parts, and pretending otherwise doesn’t help you. But your social circle is not just background noise — it’s a habit you practice every day, whether you notice it or not.
A longitudinal study of adults recovering from alcohol dependence found what you probably already sense: the more recovery-supportive people in your network, and the fewer heavy drinkers, the better your drinking outcomes over time. A separate long-term analysis showed the same pattern for perceived social support — more of it linked to less drinking and better psychological well-being across follow-ups. This isn’t about ranking your friends or writing anyone off. It’s about noticing who you spend real time with, and slowly tilting the ratio.8,9
What that looks like on a Tuesday: you skip the after-work stop with the coworker who always ends up at the bar. You accept the coffee invite from the person from group. You mute — not block, just mute — the thread that keeps pulling you back to old plans. You call your sister on the drive home instead of scrolling. Small trades. You don’t have to make a dramatic announcement. Some relationships will fade naturally as your Tuesdays fill up with different people. Some you’ll need to hold at a distance for a while, and that grief is real. Name it. Then keep going.
Peer Support, Sponsors, and Mutual-Help Groups You Might Not Have Considered
The other half of your people question is who you’re adding. A systematic review of peer support in substance use disorder recovery — recovery coaches, peer-led groups, mentors who’ve walked this before you — found peer involvement linked to better treatment engagement, reduced substance use, and stronger social outcomes. Translation: having someone in your corner who gets it, without you having to explain, does real work.10
Alcoholics Anonymous and other 12-step groups help a lot of people, and if a meeting near you in Portland or Milwaukie clicks, go back. But research comparing 12-step groups to alternatives acknowledges what you may already have felt: many people never engage with 12-step, or find they don’t feel at home there. That’s not a personal failure. There are other doors. SMART Recovery uses tools grounded in cognitive-behavioral thinking. Refuge Recovery leans on Buddhist-influenced practice. Women for Sobriety, Life Ring, and secular meetings exist too, in person and online. Alumni groups — the kind Pacific Crest Trail Detox keeps running for people after they leave — give you a room full of people who knew you at your rawest and still show up.5
Try one this week. If it doesn’t fit, try another next week. A sponsor or peer mentor is someone you can text at 9 p.m. when the craving isn’t loud yet but is definitely there. That single text — sent early, not after — is the habit. You don’t have to earn the right to reach out. Reaching out early is the practice.
Coping Skills You Can Practice in Ten Minutes
Cravings do not politely schedule themselves for therapy hours. They show up in the checkout line at Fred Meyer, in the parking lot after a hard meeting, at 4 p.m. on a Sunday when the week ahead looks too long. What helps is having a few short practices you can pull out anywhere, without needing a quiet room or a whole hour.
A randomized trial of people in aftercare compared two structured coping approaches — mindfulness-based relapse prevention and standard cognitive-behavioral relapse prevention — against treatment as usual. Both groups did better than usual care at six months, with lower relapse risk and fewer days of use. At twelve months, the mindfulness group kept pulling ahead, with fewer days of use and less heavy drinking. The takeaway isn’t that one approach beats the other. It’s that practicing something — a repeatable skill you can run in your head or on your feet — changes the odds.6
Try this the next time a craving lands. Set a timer for ten minutes. Name what you’re feeling out loud, even if it sounds silly: “I’m anxious, my chest is tight, I want to numb this.” Then do one thing with your body. Cold water on your wrists. A walk around the block. Four slow breaths where the exhale is longer than the inhale. The craving is a wave, not a verdict — you’re waiting it out, not defeating it.
Keep a short list on your phone of practices that have actually worked for you, not the ones that sound good in a workbook. Maybe it’s calling your sponsor. Maybe it’s the specific playlist that gets you through the drive home. Maybe it’s the honesty of texting your therapist, “Bad afternoon, can we talk Thursday?” 1. This is the coping habit: not white-knuckling, but reaching for a tool early, before the wave gets tall. Ten minutes is often all it takes to be on the other side of it.
Where You Live Shapes Whether You Stay
You can do everything else right and still get pulled under by the wrong roof over your head. If you’re returning to a house where someone drinks every evening, or a couch in a friend’s apartment where old plans get made at midnight, your habits are working against the room you’re in. Environment isn’t a soft variable in recovery. It’s the ground the rest of the habits have to stand on.
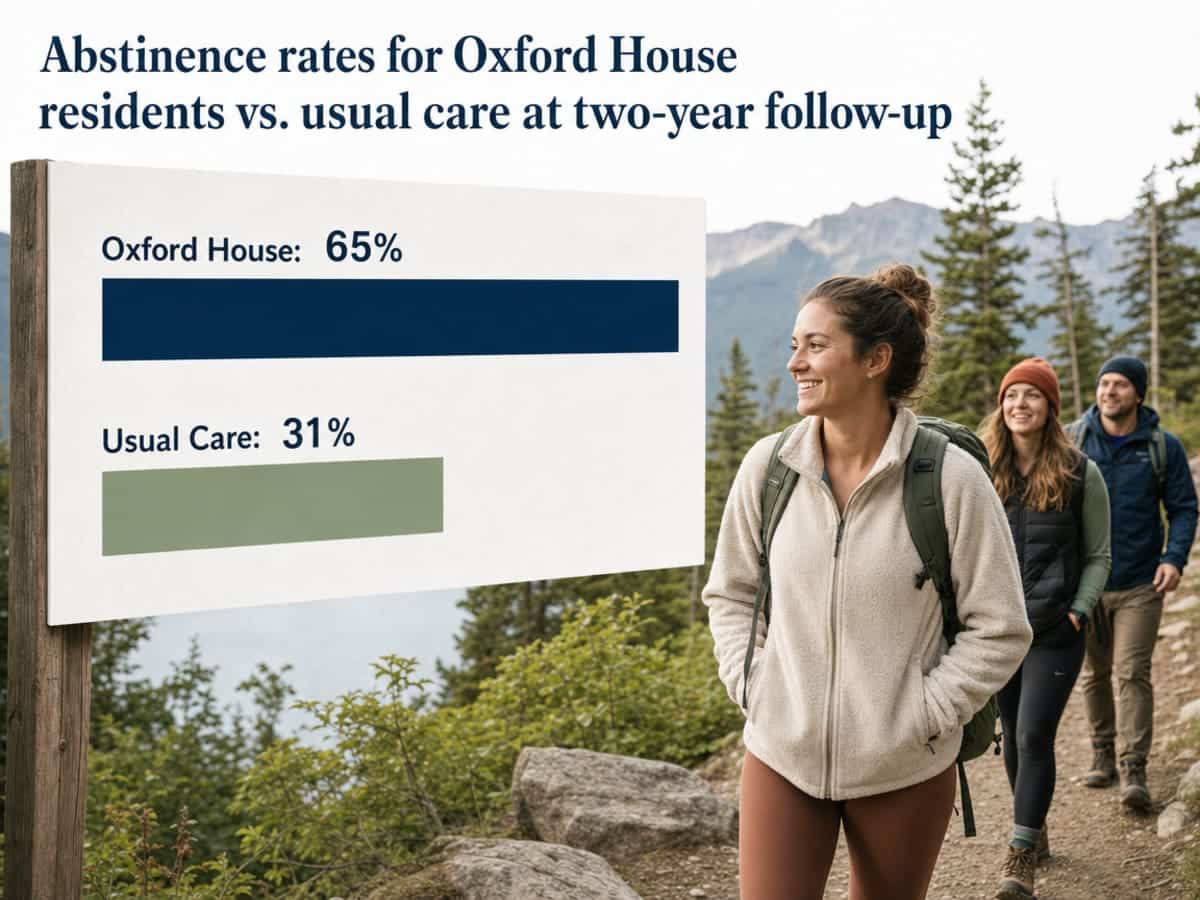
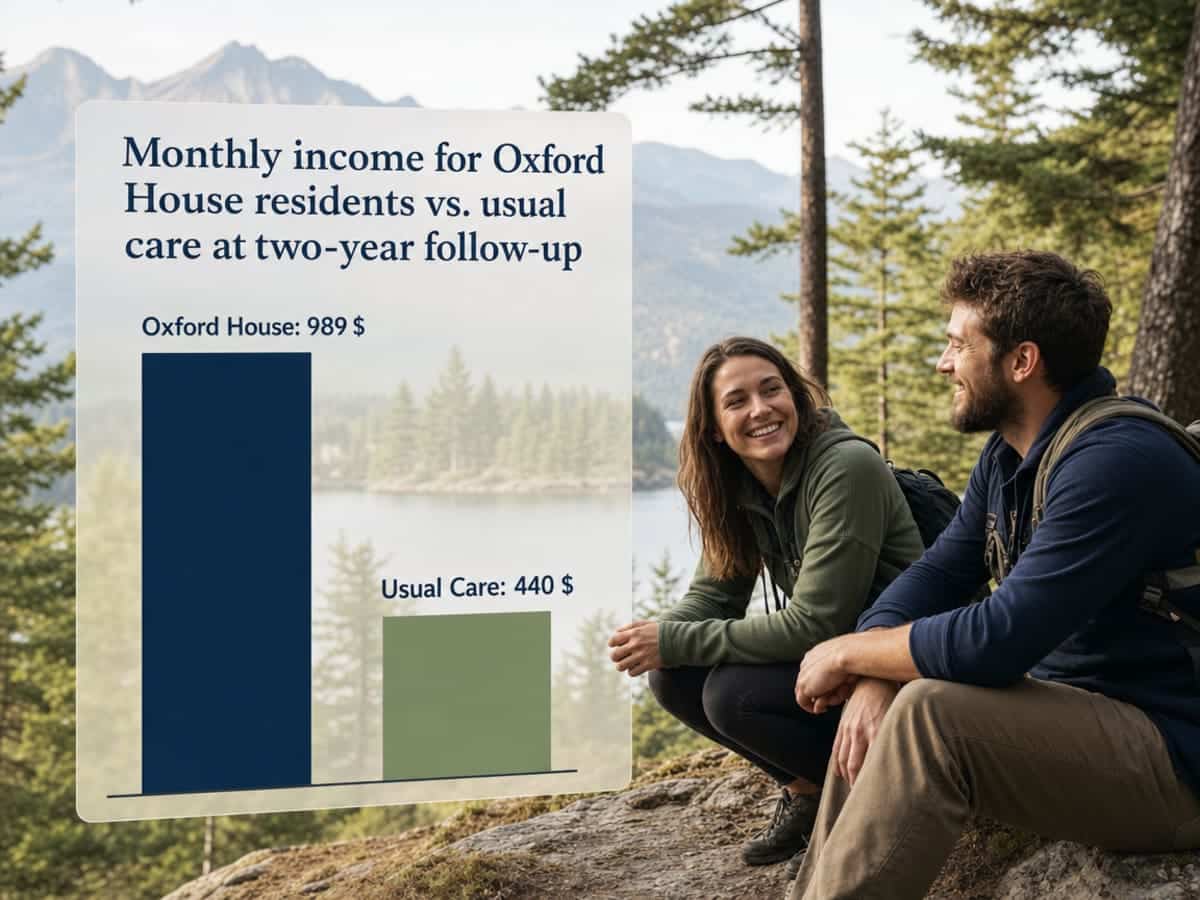
A 2025 systematic review looked at what happens when people leaving treatment move into recovery housing — sober, peer-led homes like Oxford Houses — instead of returning to unstable or use-adjacent settings. Two years later, the differences were not small.4
- Sixty-five percent of Oxford House residents were still abstinent, compared with 31 percent in usual care.
- They earned about $989 in average monthly income, versus $440.
- Their incarceration rate was 3 percent, compared with 9 percent for the usual-care group.
One environment, tracked over two years, roughly doubled the odds of staying sober and cut jail time by two-thirds.
You don’t need to land in a formal recovery house for the underlying idea to work for you. What matters is that the place you sleep is quiet, predictable, and free of the substance you’re recovering from. That might mean asking a partner to keep alcohol out of the house for a while. It might mean staying with a parent or sibling instead of returning to your old apartment. It might mean applying for a bed at a Portland-area sober living home while you finish outpatient work. None of these are admissions of weakness. They’re you being honest about what your Tuesday needs to look like to still be sober on Wednesday.
If you’re not sure what’s available near Milwaukie, Portland, or your part of the Pacific Northwest, ask. The team at Pacific Crest Trail Detox helps people plan this piece before discharge — where you’ll sleep, who else is in the house, what the first two weeks after detox actually look like — because a home-like place to land is not a bonus, it’s part of the treatment. A safe roof is the habit underneath every other habit on this list.
Movement, Meaningful Activity, and the Return of Ordinary Days
Nobody heals inside a locked room. At some point, usually before you feel ready, you need your body to move and your day to have shape. Not a gym membership or a five-year plan. A twenty-minute walk after dinner around your block in Milwaukie. A load of laundry actually folded. A shift at a job that expects you Tuesday at 9.
Researchers who study early recovery describe it as a slow redesign of daily life — building new patterns of thinking and acting that fill the space substances used to occupy. Meaningful activity is not a nice extra. It’s the thing that gives your hours somewhere to go. Work you can actually do, a class, volunteering at a food pantry, walking a neighbor’s dog, cooking a real dinner instead of eating standing up. These sound small because they are. That’s the point.12
Movement earns its own line here. You don’t need it to be athletic. A walk counts. Stretching on the living room rug counts. What matters is that your body gets to feel like your body again, not just the thing that used to crave. Pair movement with something else — a phone call to your mom while you walk, a podcast from group, the light through the trees on a Portland afternoon — and the habit sticks faster.
Ordinary days come back slowly. Let them.
Staying Tied to Care: Medication, Therapy, and the Check-In You Almost Skipped
There’s a moment, usually around month three or four, when you start to feel okay. Not great, but okay. Sleep is coming back. You’ve been to enough meetings that you know people’s names. And a small voice starts whispering that maybe you don’t need the Thursday appointment this week. Maybe you can skip the medication refill until next month. Maybe you’ve got this.
The National Institute on Drug Abuse frames recovery as a long process that often needs repeated episodes of care, with ongoing medication adherence, counseling, and peer support doing the quiet work of holding you steady. A randomized trial of people already in aftercare tested this directly. Participants in structured relapse-prevention programs — one mindfulness-based, one cognitive-behavioral — had significantly lower relapse risk and fewer days of use at six months than people getting only usual care. At twelve months, the mindfulness group kept improving, with fewer days of use and less heavy drinking than either comparison group. Staying in a structured program didn’t just help early. It compounded.3,6
If you’re on medication that steadies cravings — the kind of steadying support Pacific Crest Trail Detox helps set up during detox and hands off to outpatient care — take it the same way you’d take blood pressure medicine. Not when you feel like it. Every day. Set an alarm. Fill the pill organizer on Sunday afternoon while the coffee brews. If a side effect is bothering you, call your prescriber before you decide on your own to stop. Adjustments are normal; going quiet is what gets people in trouble.
Therapy is the same habit in a different shape. If you’re managing depression, anxiety, PTSD, or chronic pain alongside recovery, integrated care that treats both together works better than treating them separately. That means the Thursday session isn’t optional scaffolding — it’s part of the treatment. Go on the weeks you feel raw. Go on the weeks you feel fine. The check-in you almost skipped is often the one that catches the thing you didn’t know was building.14
Small Wins and the Slow Rebuild of Confidence
Somewhere in the second or third month, if you’re paying attention, you’ll notice something new. You said no to a drink at your cousin’s birthday and it wasn’t the hardest thing you did that day. You made it through a stressful meeting without your hands shaking. You cooked dinner two nights in a row. These are not small things pretending to be small. They are the actual material confidence is built from.
A meta-analysis pooling data across many studies found a consistent link between abstinence self-efficacy — your belief that you can stay sober through the next hard moment — and lower rates of substance use and relapse. Confidence isn’t a personality trait you either have or don’t. It’s evidence, stacked up over time, that you can do the thing you just did again tomorrow.13
So keep a short list. Not a gratitude journal if that word makes you cringe. Just a note on your phone where you write down one thing that went right each day. The walk you took. The call you made. The craving you sat through. Read it back on the hard days. That list is proof, and proof is what quiet the voice that says you were never going to make it anyway.
Spotting the Drift Before It Becomes a Relapse
Relapse almost never starts with a drink or a pill. It starts weeks earlier, in the small stuff you stop doing. You skip the Thursday meeting because work ran late. You skip it the next week too. You stop texting your sponsor because you’re “fine.” You start sleeping badly again and telling yourself it’s just the season. The drift is quiet, and the danger is that you only notice it once you’re already looking at old thoughts you thought you were done with.
The Five Rules of Recovery framing treats relapse as a gradual process, not a single event — an emotional stage where self-care slips, then a mental stage where you start entertaining old thinking, then the physical stage nobody wants to reach. The National Institute on Drug Abuse says the same thing in different words: if a slip happens, it’s a signal to renew care, not proof that you failed.1,3
So learn your early warning signs and write them down while things are steady:
- Skipping meetings.
- Isolating from your recovery people.
- Bad sleep two nights in a row.
- Romanticizing an old memory.
When you notice two or three stacking up, call someone that day — your therapist, your sponsor, the Pacific Crest Trail Detox alumni team. Reaching out early isn’t weakness. It’s the whole practice.
If You’re Reading This for Someone You Love
This part is for you — the spouse, the parent, the adult child, the friend who has been holding your breath for months. The rest of this article talks directly to the person in recovery. This section talks to you, because your habits shape their odds too.
Start here: you cannot want their recovery more than they do, and you cannot do the work for them. What you can do is make the environment around them a little easier to stay sober in. Keep alcohol out of the house for a while, even if it feels dramatic. Don’t ask for a daily progress report — ask how they slept, how group was, whether they need a ride Thursday. Small, specific questions land better than big ones about how they’re “really doing.”
Learn the early warning signs they wrote down when things were steady. Missed meetings. Isolating. Bad sleep. If you see two or three stacking up, say something once, kindly, and then trust their care team to do the rest. Family therapy — the kind Pacific Crest Trail Detox offers alongside detox and outpatient care — is not just for them. It’s for you, so you stop carrying this alone.1
Oregon-Specific Supports You Can Call Today
If you’re reading this from somewhere between Milwaukie and the coast, or up in Vancouver, or out past Gresham, you don’t have to figure out the next step alone. The Oregon Health Authority keeps a running list of statewide addiction services, including two numbers worth putting in your phone before you close this tab.11
- The Alcohol and Drug Help Line at 1-800-923-4357 connects you to local counselors and treatment referrals, day or night.
- The Oregon Hopeline links you to recovery mentors who have walked this themselves and can help you find meetings, housing leads, and outpatient care near you.
If you finished detox with Pacific Crest Trail Detox, the alumni team is a call away — same for family members trying to figure out what Thursday should look like. If you went through a different program, call them anyway. Nobody there will make you feel small for asking. That phone call, made today instead of next week, is the same habit this whole article has been about: reaching out early, while the ground is still steady under your feet.
Check Your Coverage—Take the First Step Forward
Quickly see if your insurance supports your recovery journey, so you can focus on lasting change.
Frequently Asked Questions
How long does it take for recovery habits to feel like second nature?
Honest answer: longer than you want, shorter than you fear. Most people notice habits like morning check-ins, meetings, and steady sleep start feeling automatic somewhere between three and six months of daily practice. Some days it will still feel like effort. That’s normal. Recovery is a long process built through repeated care and steady routine, not a single finish line.3
What should I do if I slip or relapse?
Call someone that day. Your therapist, sponsor, prescriber, or the Pacific Crest Trail Detox alumni team. A slip is a signal to renew care, not proof that you failed or wasted your work. Tell one person the truth, get back to your next meeting, and make an appointment before the week ends. Shame keeps people stuck; reaching out early is the practice that gets you moving again.3
Do I have to go to AA or a 12-step group to stay sober?
No. Twelve-step groups help many people, but research comparing them to alternatives acknowledges that a lot of people don’t engage with AA or feel at home there. SMART Recovery, Refuge Recovery, LifeRing, Women for Sobriety, secular meetings, and alumni groups all count. What matters is that you have regular peer contact — that connection is linked to better outcomes across studies. Try a few, keep what fits.5,10
How do I handle friends or family who are still using?
Slowly, and with less drama than you think. Research on recovery networks shows that having more recovery-supportive people and fewer heavy-drinking or using contacts predicts better outcomes over time. You don’t have to end relationships. You can shorten visits, skip the settings where use happens, and add new people to the mix through meetings and alumni groups. Some friendships will change. Grieve it, then keep going.9
Can I sustain recovery if I still struggle with depression, anxiety, or PTSD?
Yes, and you’ll do it more easily with both conditions treated together. Integrated care that addresses mental health and substance use at the same time leads to better psychiatric outcomes and lower substance use than treating them separately. Keep the Thursday therapy appointment. Take psychiatric medication the way it was prescribed. Tell your care team when something shifts. You are not two separate problems — you’re one whole person.14
What if I can’t sleep in early recovery?
Broken sleep is one of the most common parts of early recovery, and it matters. Research links lower sleep quality with higher drug cravings, so this is worth treating, not toughing out. Keep bedtime steady, get your phone across the room, and cut screens in the last hour. If you’re still awake at 3 a.m. for more than a few nights, tell your prescriber. There are options that help.7
References
- Relapse Prevention and the Five Rules of Recovery. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553654/
- Habits and Routines of Adults in Early Recovery From Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC9926005/
- Treatment and Recovery. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
- Recovery housing for substance use disorder: a systematic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC11922849/
- Comparison of 12-step Groups to Mutual Help Alternatives for Alcohol Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC5193234/
- Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders. https://pubmed.ncbi.nlm.nih.gov/24647726/
- Sleep quality and emotions affect opioid addiction recovery. https://www.psu.edu/news/research/story/sleep-quality-and-emotions-affect-opioid-addiction-recovery
- Social Support and Recovery from Alcohol Addiction: A Longitudinal Analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC193012/
- The role of social networks and social support in recovery from alcohol dependence. https://pubmed.ncbi.nlm.nih.gov/18497724/
- Peer support in substance use disorder recovery: A systematic review. https://pubmed.ncbi.nlm.nih.gov/28725370/
- Oregon Health Authority: Addiction Services. https://www.oregon.gov/oha/hsd/amh/pages/addictions.aspx
- Recovery from addiction: A practical model of change. https://pmc.ncbi.nlm.nih.gov/articles/PMC3673149/
- Self-efficacy and substance use outcomes: A meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC3177766/
- Integrated treatment for co-occurring disorders: Efficacy and models. https://pmc.ncbi.nlm.nih.gov/articles/PMC2951963/


