
Key Takeaways
- A treatment center is a licensed, staffed facility offering structured care for substance use or mental health, ranging from outpatient clinics to residential homes to psychiatric hospitals.1
- The right level of care depends on what your body is doing, not willpower. Daily alcohol use, benzodiazepine dependence, or prior withdrawal seizures point toward 24-hour medical supervision.7
- Non-hospital medical detox offers a home-like residential setting with around-the-clock nursing, a prescribing provider, and locked medications, sitting between hospital wards and unsupervised social detox.10
- Detox alone is not complete treatment. A good center already has the next step lined up, whether that is residential, PHP, IOP, or ongoing outpatient and aftercare.12
If You’re Reading This With Shaky Hands
If you are reading this with shaky hands, or with a knot in your stomach at 2 a.m. while someone you love sleeps badly in the next room, you are already doing something hard. You are looking.
That counts.
You probably typed “treatment center definition” because somewhere between the sweating, the racing thoughts, or the third missed day of work, you realized you need a real place with real people who know what they are doing. Not a TV version. A real one.
Here is what this article will do for you. It will explain, in plain words, the true treatment center definition, what a treatment center actually is, and what kinds exist. It will help you tell the difference between a place that can keep you medically safe during withdrawal and a place that cannot. And it will help you figure out, today, which kind of setting fits where your body and life are right now.
You do not need to understand every clinical term to make a safe next move. You need enough to ask the right question on the phone. That is what we are building here, together, one short section at a time.
Take a breath. Keep reading.
What a Treatment Center Actually Is
A treatment center is a licensed place where people get structured help for substance use, mental health, or both. That is the short version.
The longer version matters more to you right now. “Treatment center” is an umbrella word. It covers a range of facilities, from outpatient clinics where you visit a few hours a week, to residential homes where you sleep, eat, and heal under medical supervision, to psychiatric hospitals for the most intensive care. The same phrase can point to very different rooms, schedules, and levels of safety.1
What ties them together is this: a real treatment center is licensed or certified by a government agency, and it provides services aimed at changing the patterns that are hurting you, while managing the physical side of dependence when your body needs that help too. Therapy. Medicine, when medicine is the right tool. Group support. A team that knows what they are doing.13
Federal rules even spell some of this out. The Medicare manual, for example, defines inpatient psychiatric facilities with specific staffing and documentation standards. States layer their own definitions on top, especially for residential and detox programs. You do not need to memorize any of that. You just need to know that the word “center” should mean something verifiable, not a vibe.17
So when you hear “treatment center,” think: licensed, staffed, and built around a specific level of care. The next question is which level fits you.
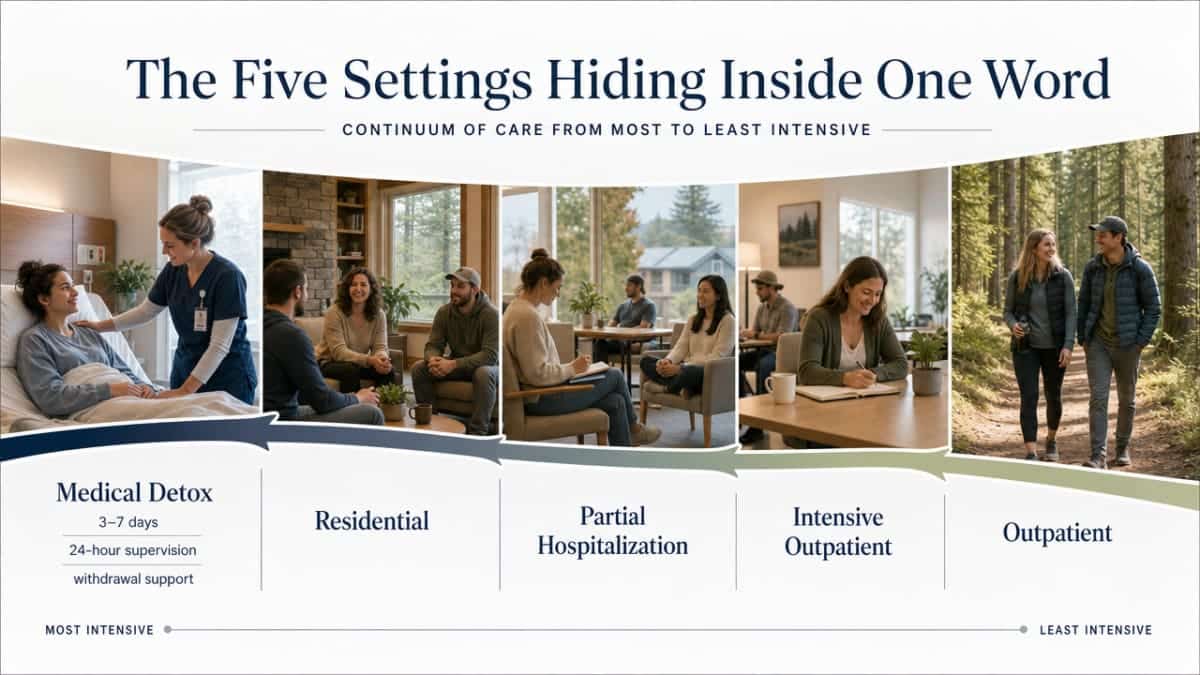
The Five Settings Hiding Inside One Word
Medical Detox: The First 3 to 7 Days
Medical detox is where you go when your body is the loudest problem in the room.
It is a short stay, usually three to seven days, where a clinical team watches over you around the clock while the substance leaves your system. Nurses check your blood pressure. A doctor or nurse practitioner prescribes medicine that takes the edge off withdrawal so your body can settle. You sleep, eat when you can, and let people who do this every day handle the parts you cannot handle alone.
The federal and state language for this is technical, but the idea is simple. Inpatient detox provides 24-hour supervision, observation, and support for patients who are intoxicated or experiencing withdrawal. New Jersey, for example, calls non-hospital medical detox a residential substance use disorders treatment facility designed primarily to provide short-term medical care. Translation: a house or small building, staffed day and night, where the whole point is to get you through withdrawal safely.7,10
The choice between hospital detox and non-hospital medical detox depends on your medical risk, your withdrawal severity, and what kind of support you have at home. If you have a heart condition, a seizure history, or you are using several substances at once, a hospital-level program may be the right call. For many people, a non-hospital medical detox with on-site nurses and a prescribing provider is enough, and it feels far less clinical.9
Detox is not the cure. It is the runway. It gets you stable enough to do the real work next.
Residential Treatment: Living There While You Heal
After detox, some people step into residential treatment. You sleep at the facility. You eat there. Therapy happens during the day, in groups and one-on-one, and the schedule is built so that your whole week points toward recovery instead of toward the next drink or pill.
States define residential treatment in slightly different ways, but the spine is the same. New Hampshire describes it as a place where paid staff provide clinical services, with 24-hour structure and staff available as needed. Utah regulates Residential Treatment Programs for groups of four or more, with specific rules for both mental health and substance use programs. Connecticut frames intermediate and long-term residential treatment as structured, supervised care for people with substance use disorders.4,5,11
What does that mean for you? It means a real bed, real meals, and a real team. Group rooms with couches and tissues. A nurse station down the hall. Counselors who lead sessions on what triggered your use and what to do when those feelings come back.
Residential makes the most sense when home is not safe for healing yet, when prior outpatient attempts have not held, or when your substance use was severe. A systematic review of inpatient and residential programs for alcohol use disorder found that this kind of structured care can improve drinking outcomes, especially for people with high severity or earlier outpatient attempts that did not stick 19. It is not failure. It is a heavier tool for a heavier load.
PHP and IOP: Structured Days, Your Own Bed at Night
PHP stands for partial hospitalization program. IOP stands for intensive outpatient program. Plain English: you go to treatment during the day, then you go home to sleep.
PHP is the more intensive of the two. Most programs run five or six days a week, several hours each day. You get group therapy, individual sessions, medication management if you need it, and a tight schedule that keeps your week from drifting. SAMHSA and NIDA materials describe partial hospitalization as a bridge between residential and outpatient care, matching people who need a lot of structure but are stable enough to live at home.7
IOP is lighter on hours but still serious. Often three days a week, three hours at a time, sometimes in the evening so you can keep working. It is built for people who have stabilized but still need group support, accountability, and skills practice.
Both fit when you have a safe place to go each night. A partner who is sober. A parent’s spare room. A home that does not have triggers waiting in every cabinet. If you cannot say yes to that, a residential program may still be the better call. PHP and IOP work because the hours away from the chair are spent rebuilding the rest of your life, not battling it alone.
Outpatient and Aftercare: The Long Tail of Staying Well
Standard outpatient is the lightest layer. Maybe one therapy session a week, plus a check-in with a prescriber if you are on medication for cravings or co-occurring depression or anxiety. The clinical guidance is straightforward: effective treatment combines medications, behavioral therapies, and recovery supports across different settings.8
Aftercare and alumni programs sit alongside outpatient. Think of them as the part where you stay connected after the intense months end. Peer groups. Sober social events. A phone number you can call when a hard week hits. NIDA’s research-based guide is direct about why this matters: treatment has to help people stop using, stay stopped, and build a real life at home, at work, and with the people they love.15
Recovery is not a 30-day project. The light layer is what keeps the heavier work from unraveling.
Matching the Setting to the Risk in Your Body
Here is the quiet truth that most articles skip: the right level of care is not about willpower or how much you want to quit. It is about what your body is doing right now.
So how do you tell where you land? Look at the signals your body and history are already giving you.
- You drink daily or near-daily, and the shakes start when you stop. Alcohol withdrawal can escalate fast, and it can be life-threatening. This is a 24-hour supervision situation 7.
- You take benzodiazepines like Xanax, Klonopin, or Ativan regularly. Benzo withdrawal carries seizure risk. You do not taper this one alone in a kitchen 9.
- You have had a withdrawal seizure before, or a close call. Your nervous system has already shown its hand. Inpatient is the safe answer.
- You use opioids heavily every day, including fentanyl or high-dose prescription painkillers. Withdrawal is rarely fatal on its own, but it is brutal, and dehydration plus relapse risk make medical support a real help.
- You are mixing substances, or you have a serious medical condition like heart issues, diabetes, or a recent injury. More variables means more reason for a clinical team.
- You are dealing with heavy depression, panic, or suicidal thoughts on top of the substance use. Co-occurring symptoms need a setting that can hold both at once 9.
- Home is not safe for healing. If your living situation is full of triggers, conflict, or other people using, a residential setting buys you the quiet your body needs.
If you nodded at even one of those, that is not a failure. That is information. It tells you a 24-hour setting is probably the right starting point, not a luxury. And if none of those fit you, an outpatient or IOP track may be enough. Either way, the body gets a vote, and listening to it is the first act of recovery.
What a Non-Hospital Medical Detox Actually Looks Like
Most people picture detox the way TV shows it. White hallways. Locked doors. A clipboard nurse and a beeping monitor. That is one version. It is not the only one, and for many people, it is not the one that fits.
A non-hospital medical detox is, in regulatory language, a residential substance use disorders treatment facility designed primarily to provide short-term medical care for withdrawal. In everyday language: it is a house, or something close to a house, where people sleep, eat, and get through the worst days of withdrawal with a clinical team on shift around the clock.10
Picture walking in. There is a living room with couches, not a waiting room with plastic chairs. Bedrooms with real beds and dressers, often shared with one other person, sometimes private. A kitchen where someone makes meals. A common area where group sessions happen on couches or around a table.
Then picture the parts you cannot see at first. A nurse station, staffed day and night. A medication cart, locked, where the nurse pulls what your prescriber ordered for withdrawal symptoms, cravings, sleep, and nausea. A small office where a doctor or nurse practitioner meets with you to adjust your plan as your body changes day to day. A counselor’s room for one-on-one talks once the worst of withdrawal eases.
State rules require this kind of staffing, not just the cozy furniture. New Hampshire, for example, defines residential treatment as a place with paid staff who provide clinical services, 24-hour structure, and staff available as needed. That phrase, “available as needed,” is doing a lot of work. It means someone is there when you wake up at 3 a.m. shaking, when your blood pressure spikes, when you cannot keep water down.4
What it is not: an unsupervised “social” detox where people just ride it out together. What it is also not: a psychiatric hospital ward with locked units and standard-issue gowns.
It is somewhere in between, and on purpose. The home-like setting matters because your nervous system is already overwhelmed. A softer room can lower the volume on everything you are feeling while the clinical team handles what your body cannot.
Why Licensing Is the Quiet Thing That Matters Most
When you are looking for a place at 2 a.m., the word “licensed“ can feel like background noise. It is not. It is the single thing that separates a real treatment center from a building with a logo.
A license means a state agency has actually looked at the place. Staffing ratios. Medical oversight. Safety protocols. Fire codes. The rules differ from state to state, but the bones are the same: a treatment center has to prove it can do what it says it does, with the people and the protocols to back it up.
Here is what that looks like in plain terms, pulled from a handful of state codes:
- New Hampshire requires residential treatment to have paid staff providing clinical services, 24-hour structure, and staff available as needed. “Available as needed” is the part that matters when you wake up shaking at 4 a.m.4
- Utah regulates Residential Treatment Programs serving four or more people, with separate rule sets for mental health and substance use programs. The size and service mix are not casual choices; they are written down.5
- Connecticut defines private freestanding facilities for substance use care, including specific requirements for intermediate and long-term residential treatment in structured, supervised settings. That is the legal floor for what “residential” can mean.11
- New Jersey defines non-hospital medical detox as a residential substance use disorders treatment facility designed primarily to provide short-term medical care. The word “medical” is the load-bearing one.10
You do not have to memorize state codes. You just need a fast way to check the place you are calling. The SAMHSA 2024 National Directory only lists facilities that are licensed, certified, or otherwise approved for inclusion by their state substance abuse agency. If a center is in the directory, a real agency has signed off. If a center will not tell you who licenses them, or dodges the question, that is your answer.16
One honest note: licensing is not a guarantee of perfect care. Federal reviews have documented serious problems even in licensed facilities, including cases where harm prompted regulatory action. But unlicensed is worse, every time. Ask. Verify. Then make the call.6
Detox Alone Is Not the Whole Treatment
Here is the part nobody likes to say out loud when you are this scared and this tired: getting through detox is not the same as getting better.
Detox is the first stage. It is the part where the substance leaves your body and a clinical team keeps you safe while that happens. The federal guidance is clear-eyed about this. Detoxification alone does not constitute complete treatment, and it should be followed by entry into ongoing care. SAMHSA frames the goal of treatment the same way: change the thoughts and behaviors that drive use, and manage physical dependence when your body needs that help. The body part is detox. The thoughts-and-behaviors part is everything that comes after.12,13
Why does this matter for the decision you are making tonight? Because if you walk out of a detox bed on day six with no plan, the same brain and the same living room and the same Tuesday afternoon are waiting for you. The substance is gone. The reasons are not.
The research-based guidance is direct about what real recovery has to do. It has to help people stop using, stay stopped, and rebuild a real life at home, at work, and with the people they love. That kind of change does not happen in a week. It happens in months of group therapy, individual counseling, medication when medication helps, and the slow practice of new habits.15
So when you call a treatment center, ask one question: what happens after detox? A good place will already have an answer. A residential bed, a PHP slot, an IOP schedule, an alumni group. The handoff matters as much as the first night.
How to Pick the Right Starting Point in the Next 24 Hours
You do not need a perfect plan. You need a safe next step, made in the next day or so, while the part of you that is willing to ask for help is still awake.
Here is a way to think it through without spiraling.
-
Start with the body. If you are drinking daily, using benzos like Xanax or Klonopin, or you have had a withdrawal seizure before, your starting point is a setting with 24-hour medical supervision. That is a hospital detox or a non-hospital medical detox with on-site nurses and a prescribing provider. Not an outpatient clinic. Not white-knuckling it at home.7
If your use is heavy opioids, including fentanyl, the body risk is different but the support need is real. Medical detox makes withdrawal survivable instead of just brutal.9
-
Then look at home. Is there someone sober nearby? Is the place you sleep relatively calm? If yes, a non-hospital residential detox followed by PHP or IOP may fit. If home is full of triggers or other people using, lean toward staying somewhere with beds, at least for the first stretch.19
-
Then make two calls. Call a licensed center directly. Ask three things: Are you licensed in this state? Do you have a bed or an opening tonight or tomorrow? What happens after detox ends? If they cannot answer those clearly, call the next one. You can also search the SAMHSA national directory, which only lists facilities approved by their state agency.16
If you live in or near the Portland metro area, Pacific Crest Trail Detox is one of those calls you can make. Either way, the goal tonight is one phone call, one honest conversation, and one bed held for you tomorrow. That is the whole assignment. You can do that.
Check Your Coverage for Detox and Care
Find out if your health insurance supports your next steps toward safe, medically supervised recovery.
Frequently Asked Questions
What is the difference between a treatment center and a rehab?
In everyday talk, people use the words the same way. “Rehab” is the shorthand. “Treatment center” is the umbrella term that covers many kinds of licensed places, from outpatient clinics to residential homes to psychiatric hospitals. So a rehab is almost always a treatment center. A treatment center is not always what most people picture when they say rehab. The thing that matters is the level of care inside, not which word the sign uses.1
How long does someone usually stay in a medical detox?
Most medical detox stays run about three to seven days, depending on what substance is leaving the body and how the person is responding. Alcohol and benzodiazepine withdrawal can stretch longer because the nervous system needs more time to settle. The clinical team adjusts day by day. Detox is the first stage, not the whole treatment, so a good program will already be lining up your next step before you leave the bed.12
Is alcohol or benzodiazepine withdrawal really dangerous enough to need a treatment center?
Yes. This is not dramatization. Alcohol and benzodiazepine withdrawal can cause seizures and other serious medical events, which is why federal guidance describes inpatient detox as a 24-hour supervised setting for people who are intoxicated or in withdrawal. The choice of setting depends on your medical risk, how severe the withdrawal is, and what support you have at home. If you drink daily or take benzos regularly, please do not taper alone. Call a licensed center.7,9
How can I tell if a treatment center is actually licensed?
Ask directly on the phone: “Who licenses or certifies you, and in what state?” A real treatment center will answer in one sentence. You can also check the SAMHSA 2024 National Directory of Drug and Alcohol Use Treatment Facilities, which only lists places licensed, certified, or otherwise approved by their state substance abuse agency. If the center will not say, or the answer feels slippery, that is your signal to call the next one on your list.16
Do I have to go to a hospital, or can detox happen somewhere more home-like?
You do not have to go to a hospital for every detox. Non-hospital medical detox is a recognized category. New Jersey, for example, defines it as a residential facility designed primarily to provide short-term medical care for withdrawal. In practice, that looks like a house with bedrooms, common rooms, and a clinical team on shift around the clock. If your medical risk is very high, hospital-level care is safer. For many people, the home-like setting fits.9,10
What happens after detox ends?
After detox, the work shifts from your body to your habits and your life. That usually means stepping into residential treatment, a partial hospitalization program, an intensive outpatient program, or standard outpatient therapy, depending on what fits. Aftercare and alumni groups keep you connected for the long stretch. Real recovery means stopping use, staying stopped, and rebuilding life at home, at work, and with the people you love. A good detox already has the next step planned.15
References
- Where is MHSUD Treatment Available?. https://behavioralhealth.chir.georgetown.edu/where-is-mhsud-treatment-available/
- DEPARTMENT OF HEALTH & HUMAN SERVICES – CMS S&C-07-15 (Psychiatric Residential Treatment Facilities). https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/downloads/SCLetter07-15.pdf
- Psychiatric Residential Treatment Facility Providers. https://www.cms.gov/medicare/health-safety-standards/certification-compliance/psychiatric-residential-treatment-facility-providers
- New Hampshire Summary – State Residential Treatment for Behavioral Health Conditions. https://aspe.hhs.gov/sites/default/files/2021-08/StateBHCond-NewHampshire.pdf
- Utah Summary – State Residential Treatment for Behavioral Health Conditions. https://aspe.hhs.gov/sites/default/files/2021-08/StateBHCond-Utah.pdf
- State Residential Treatment for Behavioral Health Conditions: Regulation and Policy – Environmental Scan. https://aspe.hhs.gov/reports/state-residential-treatment-behavioral-health-conditions-regulation-policy-environmental-scan-0
- 2 Settings, Levels of Care, and Patient Placement (TIP-related chapter). https://www.ncbi.nlm.nih.gov/books/NBK64109/
- Treatment | National Institute on Drug Abuse (NIDA). https://nida.nih.gov/research-topics/treatment
- Chapter 3 – Settings, Levels of Care (TIP 45 adjunct chapter). https://www.ncbi.nlm.nih.gov/books/NBK64812/
- N.J. Admin. Code § 8:111-1.3 – Definitions. https://www.law.cornell.edu/regulations/new-jersey/N-J-A-C-8-111-1-3
- Sections 19a-495–570: Private Freestanding Facilities for the Care or the Treatment of Substance-Abusing or Dependent Persons (Connecticut). https://portal.ct.gov/-/media/Departments-and-Agencies/DPH/dph/public_health_code/Sections/19a495570PrivateFacilitiesforSubstance.pdf
- 1 Introduction to Detoxification and Substance Abuse Treatment (TIP-related chapter). https://www.ncbi.nlm.nih.gov/books/NBK64108/
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Chapter 5—Specialized Substance Abuse Treatment Programs. https://www.ncbi.nlm.nih.gov/books/NBK64815/
- Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- 2024 National Directory of Drug and Alcohol Use Treatment Facilities. https://www.samhsa.gov/data/report/2024-national-directory-drug-and-alcohol-use-treatment
- Medicare Benefit Policy Manual, Chapter 2. https://www.cms.gov/regulations-and-guidance/guidance/manuals/downloads/bp102c02.pdf
- Residential Treatment for Substance Use Disorders: A Review of Clinical Effectiveness, Cost-Effectiveness and Guidelines. https://pubmed.ncbi.nlm.nih.gov/26763784/
- Inpatient and residential treatment of alcohol use disorder: A systematic review. https://pubmed.ncbi.nlm.nih.gov/31811935/


