Key Takeaways
- Outpatient detox is medically supervised withdrawal where someone sleeps at home, attends daily clinic check-ins, receives medication if needed, and gets group and individual counseling.
- Clinical fit depends on four factors: mild-to-moderate withdrawal risk, a stable home, adequate social support, and no major untreated medical or psychiatric conditions 4.
- Substance matters enormously — opioids often fit outpatient well with buprenorphine, while severe alcohol withdrawal and benzodiazepine tapers usually require higher-level care or specialized oversight 9, 12.
- Detox is only step one; lasting change requires continuing into PHP, IOP, or standard outpatient treatment, since withdrawal management alone does not treat the underlying disorder 6, 13.
If You’re Reading This at 1 a.m., Start Here
You’re probably sitting somewhere quiet right now. Maybe the kitchen. Maybe the edge of the bed with the door closed. Something happened tonight, or last week, or has been happening for months, and you’ve finally typed the words “outpatient detox” into a search bar because the idea of your partner going to a hospital feels like setting off a bomb in your life — but doing nothing feels worse.
First: breathe. You’re not overreacting. You’re also not too late.
Here’s what you came here to find out, in plain language. Outpatient detox is medically supervised withdrawal that happens while your partner keeps sleeping at home. They go in for appointments, get checked by a clinician, get medication if it’s needed, and come back the same day 1. For the right person, with the right substance and a stable home, the research says it can be a safe, evidence-based way to get through withdrawal without checking into a hospital bed 4.
That word — “right” — is doing a lot of work, and the rest of this article unpacks it honestly. Some situations call for outpatient. Some absolutely do not. You deserve to know the difference before you make a single phone call.
So take this one section at a time. You don’t have to solve everything tonight. You just have to understand what you’re actually choosing between.
Is Your Partner Actually a Good Fit for Outpatient Detox?
The Clinical Criteria That Decide This for You
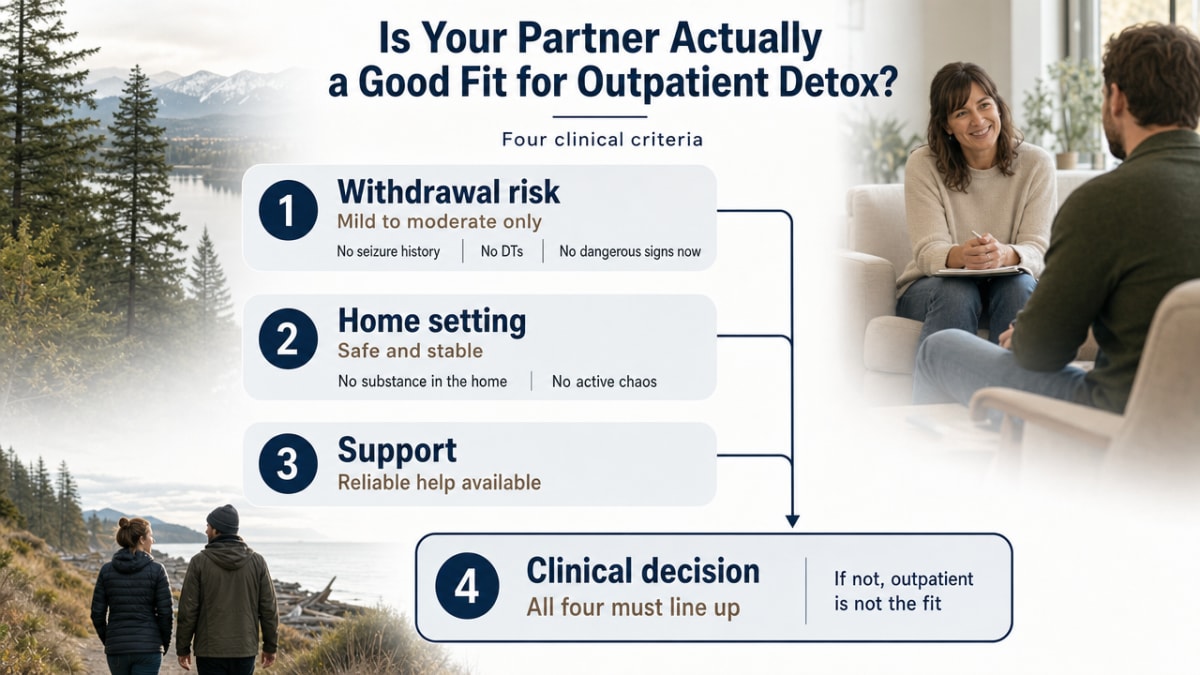
Here’s the part that surprises most spouses: outpatient detox isn’t something you pick off a menu. A clinician decides whether your partner qualifies, based on a short list of medical and home factors that have to line up. If they don’t line up, a good program will tell you so — and that’s a feature, not a rejection.
The clinical green light usually comes down to four things.
- Withdrawal risk has to be mild to moderate, not severe. That means no history of seizures, no DTs (the shakes, hallucinations, and confusion that can come with serious alcohol withdrawal), and no signs that the body is in dangerous territory already 3, 11.
- The home has to be stable enough to be a safe place to recover — meaning the substance isn’t sitting in the cupboard, there’s no active violence, and someone (usually you) can be present and paying attention 4.
- Your partner needs adequate social support, which is the clinical way of saying someone is checking on them, driving them to appointments, and noticing if something shifts.
- They can’t have major untreated medical or psychiatric conditions running alongside the withdrawal — things like uncontrolled heart problems, active suicidality, or severe co-occurring mental illness that needs its own close watch 3.
When those four boxes are checked, the research is pretty clear that ambulatory detox (the clinical term for outpatient detox — care where your partner sleeps at home) can be carried out safely and effectively in selected patients with the right medications and monitoring 4. The key word is selected. A good intake assessment is doing real work on your behalf, sorting who is safe at home and who isn’t. You want a program that takes that screening seriously, not one that says yes to everyone who calls.
When Outpatient Is the Wrong Call
This is the part of the conversation a lot of websites skip, and you deserve straight talk.
If your partner has been drinking heavily, every day, for years — especially if they’ve ever had a withdrawal seizure, a stint in the ER for shakes, or anything resembling DTs — outpatient is probably not the right starting place. Severe alcohol withdrawal can turn dangerous fast, and the safest setting for that is one with around-the-clock monitoring 11. A clinician may still get you there eventually through a step-down plan, but day one in a home bedroom isn’t usually it.
Benzodiazepines are their own category. If your partner has been taking Xanax, Klonopin, Ativan, or a similar medication regularly — even if it started with a real prescription — coming off them isn’t a quick taper. It’s often a slow, carefully monitored process that can stretch over weeks or months, because abrupt withdrawal can trigger seizures and rebound anxiety that’s worse than what they started with 9. Outpatient care can absolutely be part of a benzo taper, but it has to be the right program with real clinical oversight, not a generic detox track.
A few other situations point toward a higher level of care:
- Active suicidal thoughts
- A home where the substance is everywhere or where someone is actively using around them
- Prior detox attempts that didn’t hold
- Serious medical conditions that complicate withdrawal
None of this means your partner has failed. It means the body needs more support than four walls and a phone call can provide — and recognizing that early is one of the most protective things you can do.
What Outpatient Detox Actually Looks Like, Day by Day
A Typical Week: Morning Check-Ins, Medication, Group, Home for Dinner
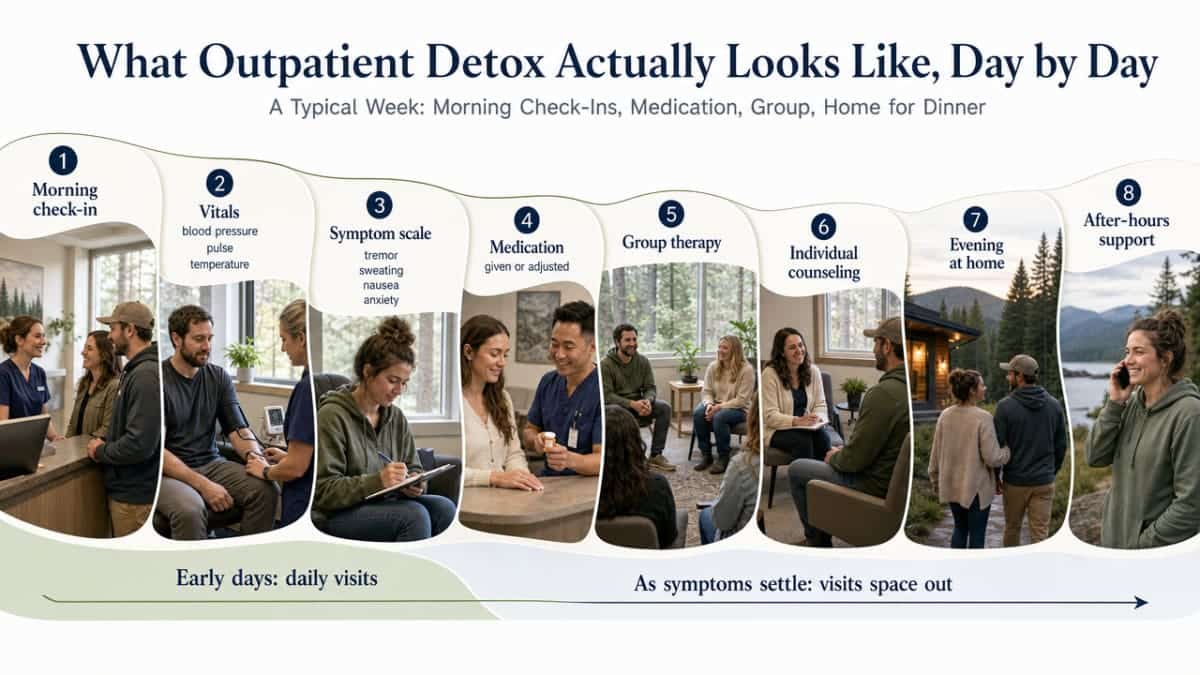
The word “outpatient” can sound vague until you see what a week actually contains. Here’s the shape of it for most people in ambulatory withdrawal management.
Mornings start with a check-in at the clinic. A nurse takes vitals — blood pressure, pulse, temperature — and walks your partner through a short symptom scale. For alcohol withdrawal, that’s usually a tool that scores tremor, sweating, nausea, anxiety, and a few other markers, so the team can tell whether things are easing, holding steady, or sliding the wrong way 11. If medication is part of the plan, it’s given or adjusted right there. Early days, especially days two through four, your partner may need to be seen daily. As symptoms settle, visits typically space out.
After the medical piece, most programs move into group therapy. This isn’t optional fluff — it’s where people learn what’s happening in their bodies, hear from others a few days ahead of them, and start building the muscles recovery actually requires. There’s usually individual counseling layered in once or twice a week, where your partner can talk about the stuff that doesn’t belong in a group room: the marriage, the job, the shame, the fear of telling their boss.
By late afternoon, they’re home. They eat dinner with you. They sleep in their own bed. If something feels off in the middle of the night — heart racing, can’t stop shaking, a craving that scares them — a good program has a clinician on call. That after-hours line is part of what makes outpatient detox safe; it’s not just business hours and a wave goodbye 4.
For opioid withdrawal, the rhythm is similar but the medication piece moves earlier — often a buprenorphine start in the first day or two that takes the edge off within hours rather than days 12. The week still has the same bones: morning medical contact, medication, group, individual work, evenings at home.
The Medications: What They Do and Why They Matter
Medication is what makes modern outpatient detox different from white-knuckling it at home. You should know what your partner might be taking and what it’s actually doing, because the words can sound scarier than the reality.
For alcohol withdrawal, the workhorse is a class called benzodiazepines — usually something like diazepam or lorazepam, given on a tapering schedule that starts higher and steps down over several days. Yes, these are the same family of drugs that can cause their own dependence problems when misused, and yes, clinicians know that. In a short, supervised taper for alcohol withdrawal, they calm the nervous system enough to prevent seizures and ease the worst of the shakes and anxiety. The evidence supports this approach as effective and safe for mild-to-moderate alcohol withdrawal in selected outpatients 4. The medication is dispensed in small amounts, not handed over as a bottle of 60.
For opioid withdrawal, the central medication is usually buprenorphine (you may see the brand name Suboxone). It’s a partial opioid agonist — meaning it activates the same brain receptors as heroin or oxycodone, but only partially and with a ceiling. The practical effect: it stops withdrawal symptoms within hours of the first dose and removes most of the craving without producing a high. Starting buprenorphine in an outpatient setting can ease withdrawal and pull your partner into ongoing treatment in a way that quitting cold turkey almost never does 12. In Oregon, buprenorphine is provided through licensed opioid treatment programs and qualified prescribers alongside counseling and supportive services 7.
You may also hear about supportive medications: something for nausea, something for sleep that isn’t habit-forming, something for blood pressure spikes. These aren’t the main act, but they make the experience humane.
Two things to hold onto. First, these medications aren’t a moral compromise — they’re treatment, the same way insulin is treatment. Second, they work best inside the structure of daily contact, counseling, and a calm place to sleep. The medicine and the support are not two separate things. They’re one thing, and that’s the whole point of outpatient detox done well.
Substance by Substance: Where Outpatient Fits, Where It Doesn’t
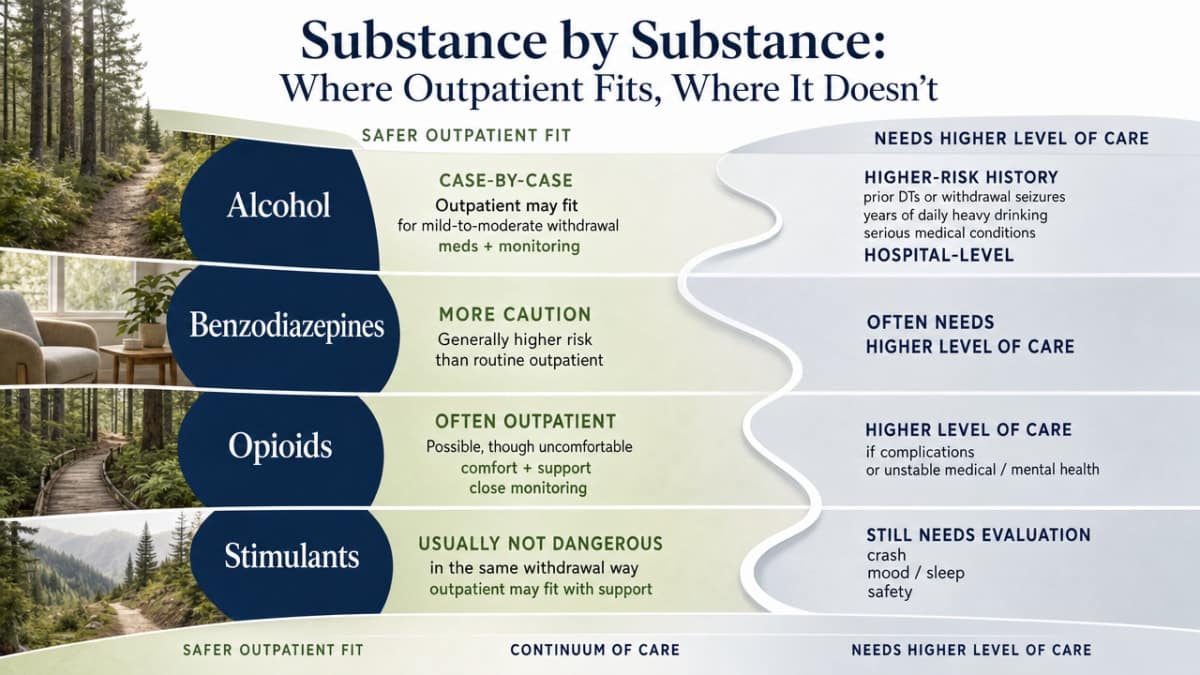
Not every substance plays by the same rules. The single biggest factor in whether outpatient detox is safe for your partner isn’t insurance or schedule — it’s what they’ve been using, how much, and for how long. Here’s a straight read on the four categories most spouses are weighing.
Alcohol: case-by-case. This is the one that most often surprises families. Mild-to-moderate alcohol withdrawal — meaning your partner drinks heavily but hasn’t had seizures, hasn’t been hospitalized for withdrawal, and doesn’t have a stack of serious medical conditions — can often be managed safely in an outpatient setting with the right medications and monitoring 11. The clinical picture changes fast, though, with daily heavy drinking over years, prior DTs, or any history of withdrawal seizures. That’s a hospital-level conversation, not a home one.
Opioids: often a strong fit. Heroin, fentanyl, oxycodone, hydrocodone, tramadol — outpatient detox is frequently the right starting place, largely because of buprenorphine. Starting buprenorphine in an outpatient setting eases withdrawal symptoms within hours of the first appropriately timed dose and pulls your partner into ongoing treatment rather than leaving them stranded after a few uncomfortable days 12. The risk of opioid withdrawal itself is mostly miserable, not life-threatening — but the risk of relapse without medication is high, which is exactly the gap outpatient MAT closes.
Benzodiazepines: high caution. Xanax, Klonopin, Ativan, Valium, and the rest of this family deserve their own paragraph because they behave differently from everything else. Coming off them is usually a slow, structured taper — sometimes stretching weeks or months — because abrupt withdrawal can cause seizures and a rebound anxiety that’s worse than the original problem 9. Outpatient care can absolutely hold this taper, but it needs a program with real benzodiazepine experience and consistent clinical contact. This is not the situation for a generic detox track or a quick weekend plan.
Stimulants: usually outpatient-appropriate. Cocaine, methamphetamine, and amphetamines don’t typically cause the dangerous physical withdrawal that alcohol and benzos can. What they cause is brutal: crushing fatigue, deep depression, intense cravings, sometimes suicidal thoughts in the first days. The medical risk is lower, so outpatient care is usually fine on that front — but the psychiatric risk needs close attention. A good outpatient program builds in daily contact during that crash window and watches mood carefully.
If your partner is using more than one substance — which is common, not unusual — the assessment leans toward the riskier one. Alcohol plus a daily Xanax habit isn’t a stimulant conversation. It’s a benzodiazepine conversation, and it deserves the caution that goes with it.
Outpatient vs. Inpatient: What the Evidence Actually Says
You may have heard, or quietly worried, that outpatient is just a cheaper, lesser version of “real” detox. That’s not what the research shows — and it’s not what experienced clinicians say either. The picture is more honest, and more useful, than that.
The phrase doing the heavy lifting there is carefully selected. Those studies didn’t pull people off the street and send them home with a prescription. They screened for mild-to-moderate withdrawal risk, a stable home, social support, and no major complicating conditions 3, 4. Inside that screened group, outpatient performed comparably on safety. Outside it, the math changes. Someone with a history of withdrawal seizures, severe daily drinking over years, or an unstable living situation belongs in a setting with around-the-clock monitoring, full stop.
So the honest comparison isn’t outpatient vs. inpatient as two equal options on a menu. It’s: which level of care fits this specific person, this specific substance, and this specific home, today? A good intake assessment answers that question for you. If outpatient is the right answer, the evidence supports it. If it isn’t, the same evidence is the reason a clinician will gently steer you somewhere else — and that steering is care, not rejection.
Detox Is Step One, Not the Whole Story
Here’s the truth that protects you from heartbreak later: getting through withdrawal is not the same as treating addiction. They’re two different jobs, and detox only does the first one.
The federal research is blunt about this. Detoxification alone does little to change long-term drug use, and patients should be encouraged to continue treatment after the acute phase ends 6. Said another way — your partner can finish a textbook-perfect outpatient detox, ring whatever metaphorical bell, and still be in real trouble two weeks later if nothing else changes. The body settles. The brain and the life around it do not, at least not yet. Detox addresses acute withdrawal but does not treat the underlying disorder 13.
So what comes next? Usually a step-down sequence inside the same outpatient world.
- Partial hospitalization (PHP) is the most intensive — several hours a day, most days of the week, mixing group therapy, individual counseling, psychiatric care, and skill-building.
- Intensive outpatient (IOP) is lighter — typically three sessions a week, often in the evening so your partner can work.
- Standard outpatient is lighter still, sometimes one weekly session, plus continued medication if MAT is part of the plan.
- Aftercare and alumni groups sit at the tail end, the place where the recovery actually has to live.
For you, that means one mental adjustment matters more than almost anything else: don’t celebrate the end of detox as the finish line. Celebrate it as the start of week one. The medical event is over. The real work — the conversations, the triggers, the rebuilding of trust at your kitchen table — is what the next several months are for.
What This Looks Like in Oregon and the Pacific Northwest
If you’re in Oregon, there’s a piece of good news worth saying out loud: the state has a real outpatient infrastructure for this, and you don’t have to figure it out alone.
For opioid use disorder specifically, medication-assisted treatment is delivered through licensed opioid treatment programs that dispense and administer methadone or buprenorphine alongside counseling, supportive services, and medical care — most of it on an outpatient basis 7. That means your partner can start buprenorphine, meet regularly with a clinician, sit in group, and still come home for dinner. The regulatory frame exists. The medication is available. The pathway from detox into ongoing MAT isn’t a maze you have to invent.
The home-like, non-hospital outpatient model that exists in the Pacific Northwest fits this picture well — medical detox without the fluorescent-light hospital experience, group therapy that feels like a room of people, and a step-down into IOP, PHP, or standard outpatient care under the same roof. That continuity matters more than most families realize on day one.
If you don’t yet know where to start, the Oregon Health Authority maintains directories of local substance use providers and runs an Alcohol and Drug Help Line for residents trying to find their connection to recovery 8. SAMHSA’s National Helpline is also free, confidential, and open 24/7, 365 days a year, with referrals to local programs including outpatient detox 10. One phone call is enough to start.
How to Take the Next Step Without Making It Bigger Than It Has to Be
You don’t have to have a plan tonight. You just need one next move.
Start with a phone screening. Most outpatient programs will talk with you or your partner for free, ask the questions a clinician needs answered, and tell you honestly whether ambulatory care is a safe starting point or whether a higher level of care is the right first step 3. That conversation is information, not a commitment. If you’re not sure where to call, the Oregon Alcohol and Drug Help Line and SAMHSA’s National Helpline are both free, confidential, and built for exactly this moment 8, 10.
Bring a few facts to the call: what your partner is using, roughly how much, for how long, any prior withdrawal episodes, any current medications, and what your home looks like on a Tuesday night. That’s enough for a real assessment to begin.
One more thing worth saying. The fact that you opened a search bar tonight, read this far, and are still here counts. It’s not nothing. It’s the first real step of a longer arc — and at Pacific Crest Trail Detox, we’ve watched a lot of families start exactly where you are.
Check Your Coverage for Outpatient Detox Today
Quickly find out if your insurance covers flexible outpatient detox options for your partner.
Frequently Asked Questions
Is outpatient detox actually safe, or are we taking a real risk by not going to a hospital?
For carefully selected people — mild-to-moderate withdrawal risk, stable home, no history of seizures or DTs — the evidence shows outpatient care can match inpatient on key safety markers like seizures and hallucinations 5. The safety isn’t in the building. It’s in the screening. A good intake decides who fits, and if your partner doesn’t, a responsible program will say so 3.
Can my partner keep working during outpatient detox?
Often, yes — but not always in week one. Early days usually mean daily morning check-ins and possible side effects from medication that make focused work hard. Many people use a few days of PTO or sick leave for the front end, then return to work as visits space out 1. Evening IOP options exist for the longer recovery work that follows detox. Honest conversation with HR isn’t always needed.
What happens if my partner relapses or uses during detox?
It happens, and a good program plans for it rather than punishing it. A slip during detox usually triggers a clinical conversation, not a dismissal — the team reassesses whether outpatient is still the right level of care or whether a step up makes sense 3. Tell the clinician. Hiding it is what makes outpatient unsafe. Honest reporting is what keeps your partner in treatment and keeps the medical team able to help.
Will insurance cover outpatient detox?
Most commercial insurance plans cover medically necessary detox and the outpatient levels of care that follow, though specifics vary by plan and program. Outpatient is generally less expensive than inpatient as a category, which matters for families weighing real budgets. The cleanest next step is a free phone screening — the intake team can verify benefits with your insurer before you commit to anything 1.
How do we handle this with the kids at home?
Match the message to the age. Young kids do well with simple, honest framing: “Dad is seeing doctors to feel better.” Older kids and teens usually already sense more than you think, and a calm, specific explanation lands better than a cover story they can poke holes in. Keep routines steady — meals, bedtime, school pickup. Predictability is what protects them. A family counselor can help script the harder conversations 2.
What do I do if I think my partner needs help but won’t go to a hospital?
This is exactly where outpatient detox earns its place. For many people, “hospital” is the wall — and an outpatient program that looks more like a clinic visit than an admission is the door that actually opens. Start with a free, confidential phone screening through SAMHSA’s National Helpline or the Oregon Alcohol and Drug Help Line 8, 10. Your partner doesn’t have to agree to treatment to agree to a conversation.
References
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Learn About Mental Health, Drug, and Alcohol Treatment. https://www.samhsa.gov/find-support/learn-about-treatment
- 2 Settings, Levels of Care, and Patient Placement. https://www.ncbi.nlm.nih.gov/books/NBK64109/
- Ambulatory detoxification in alcohol use disorder and opioid use disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC7653729/
- Summary of Evidence – Inpatient and Outpatient Treatment for Alcohol Withdrawal. https://www.ncbi.nlm.nih.gov/books/NBK507689/
- Treatment Approaches for Drug Addiction. https://nida.nih.gov/publications/drugfacts/treatment-approaches-drug-addiction
- Medication-Assisted Treatment for Opioid Use Disorder. https://www.oregon.gov/oha/hsd/amh/pages/mat.aspx
- Addiction Services – Behavioral Health Division (Oregon). https://www.oregon.gov/oha/hsd/amh/pages/addictions.aspx
- Management of benzodiazepine misuse and dependence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4657308/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- Alcohol Withdrawal Syndrome (StatPearls). https://www.ncbi.nlm.nih.gov/books/NBK424857/
- Opioid Withdrawal (StatPearls). https://www.ncbi.nlm.nih.gov/books/NBK310652/
- Substance Use Disorders (StatPearls). https://www.ncbi.nlm.nih.gov/books/NBK441882/